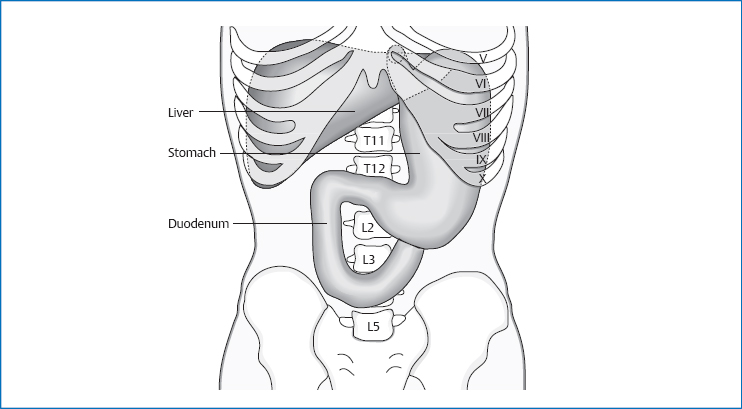
8 The Duodenum The duodenum has a total length of 25–30cm and is shaped like a horseshoe. It extends from T12 to L3, and from the right subcostal to the umbilical area. It is divided into four parts: The lumen of the duodenum narrows between the superior part and the duodenojejunal flexure from about 4.7cm to 2.7cm. This part is located about 5cm intraperitoneally. It is the most mobile part of the duodenum. Its location can vary by 4–5cm, depending on respiration, fullness of the stomach, and posture. It extends from T12 to L1. The superior part runs from the pylorus cranially, posteriorly, and to the right. Approximately 10cm long, this part is located in a secondary retroperitoneal position. It runs vertically toward caudal, more specifically to the right side of the spinal column from L1 to L3(/4). The excretory ducts of the gallbladder and pancreas enter the descending part posteromedially through the major duodenal papilla (ampulla of Vater). In addition to this common anatomy, there are numerous variations on where these two ducts can enter. An accessory pancreatic duct can enter about 2cm cranially from the ampulla of Vater, through the minor duodenal papilla (ampulla of Santorini). This part is located approximately 9cm in a secondary retroperitoneal direction. Starting from the level of L3(/4), it runs across the vertebral column slightly diagonally upward and leftward to L2. Fig. 8.1 Location of the duodenum. This part is located approximately 6cm in a secondary retroperitoneal direction. The ascending part rises from L2 to L1 cranially and to the left. It ends with a sharp angle in the duodenojejunal flexure, which again lies intraperitoneally. Fig. 8.2 Topographic relationships of the duodenum. The ligament of Treitz (suspensory muscle of the duodenum) consists of smooth and striated muscle fibers. The smooth muscle fibers originate in the superior mesenteric artery and run in a fan-shaped pattern to the ascending part, horizontal part, or duodenojejunal flexure. These fibers radiate into the longitudinal and ring-shaped muscles of the duodenum. The striated muscle fibers originate at the crus of the diaphragm and end at the duodenojejunal flexure. Along the vessels to the celiac lymph nodes. Innervation Sympathetic nervous system from T9 to T12 via the minor splanchnic nerve to the celiac plexus and the superior mesenteric plexus. Maximal time: 1–3p.m. Minimal time: 1–3a.m. Respiratory movements in the diaphragm, the varying state of fullness in the stomach, and changes in body posture can shift the duodenum as a whole, together with the head of the pancreas caudally by up to one vertebral body, in spite of the fact that it is firmly anchored in the retroperitoneal space. With increasing age, we can also see movement of the duodenum and pancreas caudally. The horizontal part can thereby extend up to the promontory. According to Barral, the superior part additionally moves toward the ascending part, as a result of which the two arms of the C-shaped duodenum approach each other. The motor of this movement is the diaphragm. In the expiratory movement, the superior part moves toward the ascending part, as a result of which the two arms of the C-shaped duodenum approach each other. In the inspiratory phase, this movement is reversed. The structure of the duodenal mucosa corresponds to the basic structure as described in Chapter 12. The circular folds (valves of Kerckring) are particularly pronounced here. One distinguishing feature of the duodenum is the Brunner glands, which produce large mucus secretions and penetrate the mucosa partly up to the layer of ring-shaped muscle. This mucus secretion contains glycopro-teins and bicarbonate to neutralize the acidic chyme. The cells of the duodenal mucosa have a short lifespan (34–38 hours), which means that we find a fast physiologic renewal of the mucosa. We can interpret this as a defense mechanism against the chyme’s acidity, because damaged cells are replaced quickly. The duodenal mucosa is therefore protected against the acidity of the stomach and the pancreatic enzymes in several ways: by the mucus produced in the Brunner glands, by the bicarbonate in the pancreatic juice, and by rapid renewal of the mucous membranes.
Anatomy
General Facts
Location
Superior Part
Descending Part
Horizontal Part
Ascending Part
Topographic Relationships
Superior Part
 spinal column: in standing position with L2 or L3, in supine position with L1 or L2
spinal column: in standing position with L2 or L3, in supine position with L1 or L2
 gallbladder
gallbladder
 liver
liver
 inferior vena cava
inferior vena cava
 head of the pancreas
head of the pancreas
 hepatoduodenal ligament
hepatoduodenal ligament
 peritoneum
peritoneum
Descending Part
 L1–L3
L1–L3
 transverse colon
transverse colon
 transverse mesocolon
transverse mesocolon
 liver
liver
 ascending colon
ascending colon
 head and excretory ducts of the pancreas
head and excretory ducts of the pancreas
 common bile duct
common bile duct
 ligament of Treitz (suspensory muscle of the duodenum)
ligament of Treitz (suspensory muscle of the duodenum)
 right kidney and renal hilum
right kidney and renal hilum
 inferior vena cava
inferior vena cava
 right ureter
right ureter
 testicular/ovarian vessels
testicular/ovarian vessels
 peritoneum
peritoneum
Horizontal Part
 L2–L3
L2–L3
 root of the mesentery
root of the mesentery
 superior mesenteric artery and vein
superior mesenteric artery and vein
 head of the pancreas
head of the pancreas
 small intestinal loops
small intestinal loops
 ligament of Treitz
ligament of Treitz
 psoas major
psoas major
 aorta
aorta
 inferior vena cava
inferior vena cava
 peritoneum
peritoneum
Ascending Part
 L1 or L2
L1 or L2
 minor tuberosity of the stomach and pylorus
minor tuberosity of the stomach and pylorus
 transverse mesocolon
transverse mesocolon
 small intestinal loops
small intestinal loops
 left psoas major
left psoas major
 ligament of Treitz
ligament of Treitz
 left kidney vessels
left kidney vessels
 aorta
aorta
 left kidney
left kidney
 peritoneum
peritoneum
 pancreas
pancreas

Attachments/Suspensions
 organ pressure
organ pressure
 turgor
turgor
 connective tissue in the retroperitoneal space
connective tissue in the retroperitoneal space
 hepatoduodenal ligament
hepatoduodenal ligament
 ligament of Treitz
ligament of Treitz
Circulation
Arterial
 gastroduodenal artery (celiac trunk)
gastroduodenal artery (celiac trunk)
 inferior pancreaticoduodenal artery (superior mesenteric artery)
inferior pancreaticoduodenal artery (superior mesenteric artery)
Venous
 portal vein
portal vein
Lymph Drainage
Organ Clock
Movement Physiology according to Barral
Mobility
Motility
Physiology
Pathologies
Symptoms that Require Medical Clarification
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


