Unicompartmental osteoarthritis of the knee is a relatively common disease that is seen in 40% of the population. Although disease isolated to the medial compartment of the knee is more common, isolated lateral disease also frequently exists (25% vs 10%). However, surgeons perform medial unicondylar knee replacement at a ratio of 10:1 when compared with lateral unicondylar knee replacement. This may be attributed to lack of familiarity or the increased difficulty of the procedure. Recent literature suggests that with proper patient selection, surgical technique, and implant choice, early survivorship ranges from 95% to 99%.
Key points
- •
Osteoarthritis isolated to the lateral compartment occurs in 5% to 10% of individuals with osteoarthritis of the knee.
- •
Varus stress radiographs are critical to identifying patients with isolated lateral compartment osteoarthritis.
- •
The fact that the lateral compartment of the knee is looser in flexion than in extension must be taken into consideration when balancing the knee.
- •
Fixed-bearing implants have a better track record in lateral unicondylar knee replacement.
- •
With proper patient selection, implant choice, and surgical technique, the lateral unicondylar knee replacement has excellent results and early survivorship.
Introduction
Osteoarthritis affecting the knee causes a significant burden on society affecting 37.4% of people 45 years of age and older and 47.8% of those 60 years of age and older. Severe tricompartmental disease is typically treated with a total knee arthroplasty (TKA), and the estimated cost associated with those hospitalizations was $28.5 in 2009. The number of TKAs performed each year is rising and is projected to hit 3.8 million procedures per year by the year 2030. However, not all degenerative joint disease affects more than one compartment.
Various studies report the rate of unicompartmental disease from 6% to 40%. Isolated medial compartment disease is seen in approximately 25% of knees with osteoarthritis, whereas isolated lateral compartment disease is only seen in 5% to 10%. Historically, femoral and tibial osteotomies have been somewhat effective in treating unicompartmental disease that does not involve full-thickness cartilage lesions; however, they have not been effective in cases with full-thickness lesions.
Unicondylar knee arthroplasty (UKA), as opposed to TKA, provides a less invasive, more conservative option to patients with osteoarthritis affecting only one of the three compartments of the knee. Studies have shown that UKA has reduced associated morbidity, a more rapid recovery, more preserved bone stock, more physiologically normal kinematics, and better postoperative range of motion compared with TKA. In addition, UKA feels closer to a native knee and has a more normal gait pattern.
Data suggest that UKA is not always being performed when indicated. Medial UKA and lateral UKA constitutes only 11% (10% and 1%, respectively) of all knee arthroplasty procedures performed, whereas the combined rate of isolated medial and lateral disease is 30% to 40%. This discrepancy may be attributed to hesitancy associated with a lack of familiarity with the procedure or failure to recognize isolated compartment disease. Furthermore, the 10:1 ratio of medial to lateral UKA could also be attributed to a lack of familiarity with the procedure and the increased difficulty of lateral UKA because of the screw-home mechanism, which complicates the kinematic profile of the lateral compartment.
There are a limited number of studies investigating the survival of lateral UKA when compared with medial UKA, but the most recent data suggest that lateral UKA can be just as effective of a procedure as the medial UKA. Outcomes hinge on proper patient and implant selection and surgical technique.
Introduction
Osteoarthritis affecting the knee causes a significant burden on society affecting 37.4% of people 45 years of age and older and 47.8% of those 60 years of age and older. Severe tricompartmental disease is typically treated with a total knee arthroplasty (TKA), and the estimated cost associated with those hospitalizations was $28.5 in 2009. The number of TKAs performed each year is rising and is projected to hit 3.8 million procedures per year by the year 2030. However, not all degenerative joint disease affects more than one compartment.
Various studies report the rate of unicompartmental disease from 6% to 40%. Isolated medial compartment disease is seen in approximately 25% of knees with osteoarthritis, whereas isolated lateral compartment disease is only seen in 5% to 10%. Historically, femoral and tibial osteotomies have been somewhat effective in treating unicompartmental disease that does not involve full-thickness cartilage lesions; however, they have not been effective in cases with full-thickness lesions.
Unicondylar knee arthroplasty (UKA), as opposed to TKA, provides a less invasive, more conservative option to patients with osteoarthritis affecting only one of the three compartments of the knee. Studies have shown that UKA has reduced associated morbidity, a more rapid recovery, more preserved bone stock, more physiologically normal kinematics, and better postoperative range of motion compared with TKA. In addition, UKA feels closer to a native knee and has a more normal gait pattern.
Data suggest that UKA is not always being performed when indicated. Medial UKA and lateral UKA constitutes only 11% (10% and 1%, respectively) of all knee arthroplasty procedures performed, whereas the combined rate of isolated medial and lateral disease is 30% to 40%. This discrepancy may be attributed to hesitancy associated with a lack of familiarity with the procedure or failure to recognize isolated compartment disease. Furthermore, the 10:1 ratio of medial to lateral UKA could also be attributed to a lack of familiarity with the procedure and the increased difficulty of lateral UKA because of the screw-home mechanism, which complicates the kinematic profile of the lateral compartment.
There are a limited number of studies investigating the survival of lateral UKA when compared with medial UKA, but the most recent data suggest that lateral UKA can be just as effective of a procedure as the medial UKA. Outcomes hinge on proper patient and implant selection and surgical technique.
Indications
Patients that are being considered for lateral UKA should have isolated lateral compartment disease radiographically and by examination. Berend and colleagues also argue that minor patellofemoral disease may also be ignored. In addition to isolated lateral compartment disease, varus and valgus stress radiographs demonstrating a correctable deformity with maintenance of the medial joint space are usually adequate for identifying isolated lateral disease. Argenson and colleagues showed improved long-term survivorship after adopting the practice of evaluating opposite femorotibial compartment and the flexibility of the deformity using stress radiographs.
Surgical technique of lateral unicondylar knee arthroplasty
The senior author uses an extramedullary tibial guide and an extramedullary femoral guide following implant techniques according to the implant manufacturer’s technique guideline. The components include a spherical femoral component with a nonmodular, metal-backed, fixed-bearing tibial design. A fixed-bearing device for lateral UKA is recommended because of the high range of motion, femoral posterior subluxation, screw-home mechanism, and significant laxity of the lateral compartment in flexion. A summary of the surgical technique used at our institution is described next.
Positioning
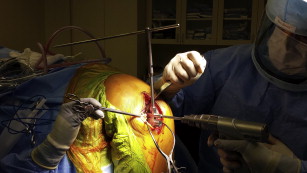
The patient is placed supine on a standard operating table with a tourniquet placed on the proximal thigh. The operative leg is placed in a hanging leg position with a leg holder on the side of the bed. This leg holder is positioned so the hip is flexed 30 degrees and 135 degrees of knee flexion without impingement on the side of the bed ( Fig. 1 ). The nonoperative leg is placed in a padded leg holder, and the foot of the bed is dropped perpendicular to the floor. The leg is then prepared and draped.

Approach and exposure
An abbreviated midline incision is created from approximately 2 cm proximal to the superior pole of the patella, extending to the proximal, lateral aspect of the tibial tubercle. Through this incision, a lateral parapatellar approach is performed with careful dissection of the superficial fascia and preservation of the infrapatellar fat pad. Lateral tibial and femoral osteophytes are excised. The visible part of the lateral meniscus is excised. The front of the tibia, from the tibial tubercle to the rim of the plateau and Gerdy tubercle, is exposed. Isolated lateral disease and an intact anterior cruciate ligament are confirmed before proceeding.
Tibial cut
An extramedullary tibial guide is placed to set the varus/valgus alignment and slope. The amount of slope depends on manufacturers’ recommendations and for this system is set at 0 degrees. The patellar tendon is split in line with its fibers ( Fig. 2 ). The vertical tibial cut is the first cut made using a reciprocating saw with a stiff narrow blade. This cut should be in line with the medial border of the lateral femoral condyle and internally rotated 10 to 15 degrees from the mid-sagittal plane of the tibia ( Fig. 3 ). The transpatellar tendon technique facilitates the proper amount of internal rotation of the tibial component. This allows the femoral component to articulate with the tibial polyethylene evenly throughout the screw-home mechanism and enlarges the surface area of the resection/implant to prevent subsidence.


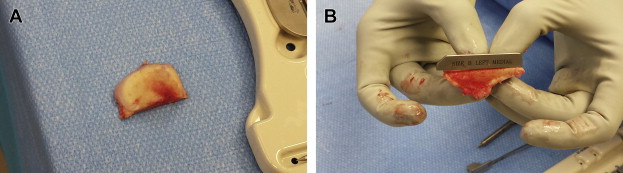
An Army-Navy type retractor is placed to protect the patellar tendon and the horizontal tibial cut is made using a 12-mm-wide oscillating saw blade ( Fig. 4 ). Enough bone must be resected to fit the tibial template and a 5-mm spacer in the flexion gap. A broad osteotome is used to lever up the resected plateau and it is excised along with the remaining soft tissue attachments posteriorly. This resected bone is matched up against the tibial baseplate trials for sizing ( Fig. 5 ).
Posterior condyle resection and milling
An extramedullary guide is used to align the femoral resections. It is aligned parallel to the anatomic axis of the femur. A tibial template is placed, the femoral drill guide is inserted, and a 4-mm spacer in between them. The drill guide ultimately sets the position of the femoral component and should be set parallel to the extramedullary guide in the axial and sagittal plane ( Fig. 6 ). A common mistake is to internally rotate the drill guide. This leads to a malpositioned femoral component resulting in impingement on the tibial spine eminence in knee extension through the screw-home mechanism. Placing the drill guide too medial similarly leads to impingement against the tibial spine eminence in extension and edge loading of the tibial polyethylene. To avoid this, the drill guide should be placed in the middle of the condyle or even cheated slightly lateral.