Chapter 8. The cervical spine
CHAPTER CONTENTS
Summary181
Anatomy 181
The joints of the cervical spine 183
Intervertebral discs 184
Cervical spinal nerves 185
Cervical arteries 186
Differential diagnosis at the cervical spine 188
Mechanical cervical lesions 188
Other causes of head and neck pain, arm pain and associated signs and symptoms 189
Cervical artery dysfunction 193
Cervical lesions – a classification system of three clinical models 203
Clinical Model 1: acute torticollis 204
Clinical Model 2 204
Clinical Model 3: presenting with referred arm symptoms 204
Treatment of cervical lesions 205
SUMMARY
Safety is of paramount importance in the application of manual techniques to the cervical spine. As a contribution to safety, this chapter begins with a summary of the key points of cervical anatomy, highlighting structures involved in the pre-treatment testing procedures and the treatment techniques themselves.
Differential diagnosis and the elements of clinical examination will be discussed. Patients with a mechanical lesion, and thus suitable for the treatments subsequently described, will be identified. The contraindications to treatment will be emphasized and guidelines for safe practice will be given, since both are of vital importance.
ANATOMY
The spinal column is a series of motion segments, each of which consists of an interbody joint and its two adjacent zygapophyseal joints. The resultant bony canal is protective, but while the structural arrangement of the lumbar spine as a whole is suited to weight-bearing, movement and stability, the cervical spine is designed principally for mobility.
The cervical spine is the most mobile area of the spine and its wide range and combinations of movement are related to changes in the direction of vision, the positioning of the upper limbs and hands, and locomotion. It is also an area of potential danger as it gives bony protection to major blood vessels that supply the brain and the spinal cord (Taylor & Twomey 1994, Nordin & Frankel 2001, Kerry & Taylor 2006).
Its mobility is at the expense of stability and it has a close neurophysiological connection to the vestibular and visual systems. It can therefore be the source of a ‘plethora of symptoms’ (Kristjansson 2005).
Anatomically and functionally, the cervical spine can be divided into two segments. The upper segment consists of the atlas and the axis (C1 and C2). Its structure is designed for mobility, with approximately one-third of cervical flexion and extension and over half of axial rotation occurring at this level (Mercer & Bogduk 2001). The lower segment consists of the remaining cervical vertebrae (C3–C7), and contributes to overall mobility.
The atlas (C1) is composed of two lateral masses, supporting articular facets, and their joining anterior and posterior arches. The superior facets articulate with the head at the atlanto-occipital joints and their condylar shape facilitates nodding movements of the head (Netter 1987, Mercer & Bogduk 2001). The inferior facets articulate with the axis at the atlantoaxial joints where rotation is the principal movement.
The axis (C2) has broad superior articular facets which support the lateral masses of the atlas and which are responsible for bearing the axial load of the head and atlas, transmitting the load to the rest of the cervical spine. The axis supports the dens or odontoid process on its superior surface, the dens providing a pivot around which the atlas rotates at the synovial median atlantoaxial joint (Mercer & Bogduk 2001). There is no intervertebral disc between the atlas and axis.
The internal ligaments of the upper cervical segment are particularly important to its stability (Fig. 8.1). The tectorial membrane is a superior extension of the posterior longitudinal ligament that covers the dens and its ligaments, acting as protection for the junction of the spinal cord and the medulla. The transverse ligament of the atlas is a strong horizontal band with extensions passing vertically and horizontally from its midpoint to form a ligamentous complex called the cruciform ligament. This, together with the apical ligament of the dens, is responsible for keeping the dens in close contact with the atlas. Any instability in the upper cervical segment, e.g. as occurs with rheumatoid arthritis, trauma or Down’s syndrome, is an absolute contraindication to orthopaedic medicine techniques.
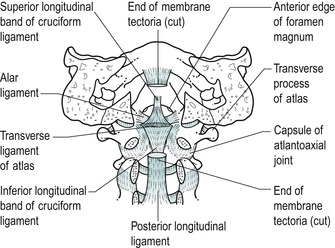 |
| Figure 8.1 Upper cervical internal ligaments. From Functional Anatomy of the Spine by Oliver J and Middleditch A. Reprinted by permission of Elsevier Ltd. |
The lower cervical segment consists of typical cervical vertebrae C3–C6 and the atypical C7 which is known as the vertebra prominens because of its long spinous process. A typical cervical vertebra consists of a small, broad, weight-bearing vertebral body (Fig. 8.2), the superior surface of which is raised on each side, rather like a bucket seat, to form unciform processes. The unciform processes articulate with corresponding facets on the vertebra above to form the uncovertebral joints or the joints of Luschka.
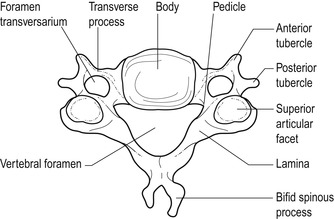 |
| Figure 8.2 Typical cervical vertebra. From Anatomy and Human Movement by Palastanga N, Field D and Soames R. Reprinted by permission of Elsevier Ltd. |
Posteriorly lie two short pedicles and two long, narrow laminae forming the vertebral arch which, together with the vertebral body, surround a large, triangular vertebral canal. The laminae come together to form a bifid spinous process. Superior and inferior articular processes, at the junction of the pedicles and laminae, articulate at the synovial zygapophyseal joints which form an articular pillar on either side of the spine.
Short, gutter-shaped transverse processes slope anterolaterally to transport the emerging nerve root. The foramen transversarium, a distinctive feature in the transverse processes on each side of the cervical vertebrae, houses the vertebral artery.
The ligaments of the lower cervical segment assist stability and allow mobility. The anterior longitudinal ligament protects the anterior aspect of the intervertebral joints and, with other anterior soft tissues, limits cervical extension. The ligamentum nuchae is a strong, fibroelastic sheet protecting the joints posteriorly and providing an intermuscular septum. The ligamentum flavum is a highly elastic ligament linking adjacent laminae. In the cervical spine it allows separation of the vertebrae during flexion and assists the neck’s return to the upright posture. Its elastic properties also allow it to return to its original length, so preventing buckling into the spinal canal where it can sometimes compromise the spinal cord.
The posterior longitudinal ligament passes from the axis to the sacrum and is at its broadest in the cervical spine where it covers the entire floor of the cervical vertebral canal, supporting the disc and possibly preventing its posterior displacement. It is taut in flexion and relaxed in extension. Mercer & Bogduk (1999) identify three distinct layers of the posterior longitudinal ligament. The deep layer, consisting of short fibres, spans each intervertebral joint and extends in an alar (wing-shaped) pattern as far as the posterior end of the base of the uncinate process, where it is believed to compensate for a deficient posterior annulus fibrosus.
The joints of the cervical spine
The joints of the lower cervical segment consist of the interbody joint anteriorly and the two zygapophyseal joints posteriorly. The interbody joint is made up of the intervertebral joint and the uncovertebral joints. When stacked, the joints can be considered to form three pillars in a triangular formation, the vertebral bodies and uncinate processes forming the anterior column and the two articular pillars formed by the zygapophyseal joints arranged posteriorly (Mercer & Bogduk 1999).
The intervertebral joint is a symphysis formed between the relatively avascular intervertebral disc and the adjacent vertebral bodies. The disc contributes to mobility and, as it ages, assists the uncovertebral joints in providing translatory glide to the movements of flexion and extension (see below).
The uncovertebral joints (joints of Luschka) are formed between the unciform processes and corresponding facets on the vertebral body above (Fig. 8.3), though their existence has been challenged (Mercer & Bogduk 1999). They may be true synovial joints or adventitious fibrous joints which have developed through clefts or fissures in the lateral corners of the annulus fibrosis of the intervertebral disc originally described by Hurbert von Luschka in 1858 (Prescher 1998). These fissures are absent in young children and appear to develop in conjunction with the development of the unciform process.
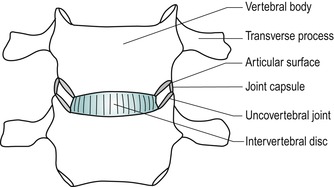 |
| Figure 8.3 Uncovertebral joints. From Anatomy and Human Movement by Palastanga N, Field D and Soames R. Reprinted by permission of Elsevier Ltd. |
Once formed, the fissures in the annulus develop a pseudocapsule in which vascularized synovial folds have been seen. Prescher (1998) relates the development of these fissures and the uncovertebral ‘joint’ to the development of the cervical lordosis resulting in a change in configuration and the magnitude of the loads transmitted through the cervical spine. This results in strong shear forces being transmitted through the intervertebral disc, particularly during rotation and side flexion. C3–C5 are the most loaded segments and it is at these levels that the fissures in the disc first appear.
The uncovertebral joints also contribute to mobility by providing a translatory gliding component to flexion and extension as well as stabilizing the spine by limiting the amount of side flexion. The gliding component produces shear which extends horizontal fissuring of the disc medially from the uncovertebral joints. This, together with the degenerative process, may eventually produce a bipartite disc (see below) (Taylor & Twomey 1994, Mercer & Bogduk 1999).
The position of the uncovertebral joints gives bony protection to the nerve root from posterolateral disc displacement. As synovial ‘joints’, degenerative changes can have an effect on the uncovertebral joints. Osteophyte formation on the uncinate process occurs predominantly in the lower cervical segments. Posterior osteophytes can encroach on the intervertebral canal leading to compression of the emerging spinal nerve root, whereas anterior osteophytes may compress the vertebral artery.
The zygapophyseal joints are synovial plane joints with relatively lax fibrous capsules to facilitate movement. The articular facets are angled at approximately 45° to the vertical so that side flexion and rotation of the lower cervical spine occur as a coupled movement. This angle of inclination adds to the component of translatory glide during flexion and extension (Taylor & Twomey 1994).
A number of intra-articular structures have been described, particularly vascular synovial folds, similar to the alar folds of the knee, as well as fat pads and meniscoid structures. All are highly innervated and can be a potential source of pain (Taylor & Twomey 1994, Oliver & Middleditch 2006). As synovial joints, the zygapophyseal joints are prone to degenerative changes and, being placed near the exiting nerve root, osteophyte formation may affect the size of the intervertebral foramen.
Orthopaedic medicine treatment was traditionally based on the discal model, but it should be remembered that any structure that receives a nerve supply can be a potential source of pain. Since the cervical spine is made up of individual motion segments, a lesion of one part of the segment will tend to influence the rest of that segment. Similarly, treatment directed to one part of a segment will affect the segment as a whole.
Intervertebral discs
There are six cervical discs which facilitate and restrain movement as well as transmit load from one vertebral body to the next (Fig. 8.4). Cervical discs are approximately 5 mm thick (Palastanga et al 2006) and the thinnest of all the intervertebral discs. Each forms part of the anterior wall of the intervertebral foramen and is thicker anteriorly, contributing to the cervical lordosis. The intervertebral disc consists of an annulus fibrosus, nucleus pulposus, and transitional superior and inferior vertebral end-plates.
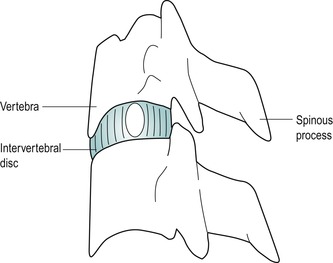 |
| Figure 8.4 Cervical vertebrae, interbody joint and posterior elements. From Anatomy and Human Movement by Palastanga N, Field D and Soames R. Reprinted by permission of Elsevier Ltd. |
The difference in function between the lumbar and cervical spine and the traditionally accepted view that cervical discs are smaller versions of lumbar discs does not hold true. Mercer & Bogduk (1999) acknowledged this in their investigation of the form of the human adult intervertebral cervical disc and its ligaments. At birth the nucleus consists of no more than 25% of the entire disc and it undergoes rapid degeneration with age so that, by the age of 30, the nucleus is undistinguishable as such.
The structure of the annulus fibrosus, described by Mercer & Bogduk (1999), is different anteriorly and posteriorly (Fig. 8.5). The anterolateral annulus forms a crescent shape when viewed from above, thicker in the median plane and thinner laterally, tapering out to the unciform processes. It forms a dense, anterior interosseous ligament. The fibres arise from the superior surface of the lower vertebra, fanning out in an alar fashion laterally, but in the midline form a tightly interwoven pattern with fibres from opposite sides, not the true laminate structure as seen in the lumbar spine. A distance of 2–3 mm from the surface of the anterior annulus, collagen fibres have been found embedded with proteoglycans and forming a fibrocartilaginous mass which has a pearly appearance and the consistency of soap.
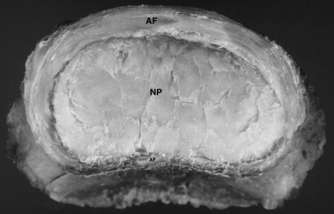 |
| Figure 8.5 Photograph showing the top view of a 39-year-old cervical intervertebral disc. The annulus fibrosus (AF) is thick and fibrous, tapering posteriorly towards the uncinate region. Posteriorly the thin annulus fibrosus (AF) is found only towards the midline. Centrally the nucleus pulposus (NP) appears as a fibrocartilaginous core. From Grieve’s Modern Manual Therapy, 3rd edn by Boyling J D, Jull G A (eds). Reprinted by permission of Elsevier Ltd. |
On a deeper plane, the fibrocartilaginous mass becomes more homogeneous and less laminated, forming what the authors interpret as the nucleus of the disc. Clefts, presumably the uncovertebral ‘joints’, are seen to extend into the fibrocartilaginous core laterally at the uncovertebral region, partially into the core in younger patients but totally transecting the posterior two-thirds of the disc in older specimens (bipartite disc). Covering the clefts in the uncovertebral region is thin periosteofascial tissue, the annular fibres being deficient here.
The posterior annulus demonstrates different features to the anterior annulus. It consists of a thin layer of one set of vertically oriented collagen fibres, not more than 1 mm thick, passing between adjacent vertebrae and extending out as far as the unciform process on each side where no oblique posterior annular fibres were found. Deep to this is the fibrocartilaginous core. It would appear that the deep layer of the posterior longitudinal ligament, with short fibres spanning each intervertebral joint, compensates for the lack of annular fibres in the posterior part of the disc, supporting the nucleus posteriorly. Posterolaterally the alar fibres of the posterior longitudinal ligament alone contain the nucleus and these may become torn or stretched by a bulging disc, or nuclear material may herniate under or through them.
The vertebral end-plate offers protection by preventing the disc from bulging into the vertebral body. It acts as a semipermeable membrane which, by diffusion, facilitates the exchange of nutrients between the vertebral body and the disc.
Cyriax (1982) stated that ‘from a clinical point of view nuclear protrusions form only a small minority of cervical disc displacements’. He postulated that a true nuclear disc lesion occurs only in adolescents and young adults, presenting as an acute torticollis. His hypothesis would seem to be substantiated by Taylor & Twomey (1994) who suggested that early degeneration of the cervical nucleus makes nuclear protrusion in the cervical spine unlikely, unless precipitated by severe trauma. A central bar-like protrusion of the annulus was more likely to occur in the cervical spine. This appeared to be refuted by the work of Mercer & Bogduk (1999) described above, given the relatively deficient posterior cervical annulus identified. Perhaps, like lumbar discs, herniated cervical discs may consist of degenerate nuclear material. Posterolateral herniation of the disc could be possible through the weak supporting alar fibres of the posterior longitudinal ligament in the uncovertebral region. Indeed, one specimen from the Mercer & Bogduk study (1999) illustrates a disc bulge and a herniation, both below their respective alar fibres.
The position of the uncovertebral joints and the large vertebral canal in the cervical spine may both also exert a protective influence on disc movement. Degenerate cervical discs may prolapse directly posteriorly, encroaching on the dura through the posterior longitudinal ligament, rather than laterally at the uncovertebral region, to affect the dural nerve root sleeve and underlying nerve root in the intervertebral canal. Alternatively, discal material may be reflected posterolaterally in the vertebral canal by the stronger median part of the posterior longitudinal ligament to cause unilateral pressure on the dura.
The triangular vertebral canal is at its largest in the cervical spine and, even though the cervical cord is enlarged in this region, there may be room for a prolapse to be accommodated. Posterolateral prolapse through the weaker alar portion in the uncovertebral region may encroach on the dural nerve root sleeve and underlying nerve root. However, it would seem that only a very large posterolateral prolapse would be able to compress the nerve root at the same level, unless there is canal stenosis caused by osteophyte formation, an infolding ligamentum flavum or congenital factors.
Since the extent of pain referral is thought to be related to the amount of pressure on the dural nerve root sleeve (Mooney & Robertson 1976), brachial pain is not as commonly associated with cervical disc lesions as sciatica is with lumbar disc lesions. Dural pressure due to a cervical disc tends to produce central or unilateral scapular pain.
It is assumed that cervical discs are innervated in a similar way to lumbar discs, since no studies have refuted this as yet. Bogduk (1994a) acknowledged the paucity of data on cervical discs but claimed that the few studies that had been done had been positive, demonstrating that the cervical discs do have an innervation. In that respect, the data on cervical discs are in accord with those on lumbar discs. At least the outer third and possibly the outer half of the annulus fibrosis receives a nerve supply from branches of a posterior longitudinal plexus, derived from the cervical sinuvertebral nerves, as well as from a similar plexus formed from cervical sympathetic trunks and the vertebral nerves, and from penetrating branches from the vertebral nerve (Bogduk 1994a). Mendel et al (1992) found evidence of nerve fibres and mechanoreceptors in the posterolateral region of the annulus.
The cervical disc may produce either primary disc pain, pain due to the mechanical effect of secondary compression of pain-sensitive structures, or pain associated with chemical or ischaemic effects. The mechanism of pain produced by disc displacement is covered in greater detail in Chapter 13 since much of the investigative work on pain production has been performed in the lumbar region and no studies have been identified that relate to the cervical spine. If findings can be extrapolated to the cervical spine, disc material is thought to undergo a process of degradation which contributes to its herniation. The chemical mediators of inflammation may play a role in the pathophysiology of cervical radiculopathy which renders the nerve root pain-sensitive (Kang et al 1995).
Cervical spinal nerves
There are eight cervical spinal nerves, each approximately 1 cm long. Each nerve, together with the dorsal root ganglion, occupies a large, funnel-shaped intervertebral foramen (Fig. 8.6). The spinal nerve is composed of one dorsal or posterior nerve root and one anterior or ventral nerve root, the ventral nerve root emerging more caudally from the dura mater (Tanaka et al 2000). The dorsal nerve root carries sensory fibres and the ventral nerve root, motor fibres.
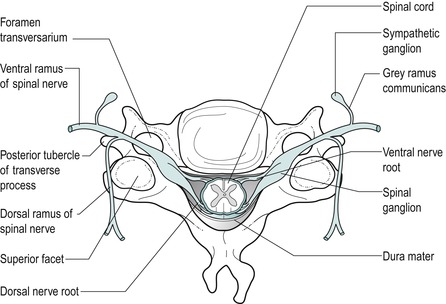 |
| Figure 8.6 Formation of a spinal nerve. From Functional Anatomy of the Spine by Oliver J and Middleditch A. Reprinted by permission of Elsevier Ltd |
The spinal nerve occupies one-fourth to one-third of the intervertebral foramen diameter and carries with it an investment of the dura mater, the dural nerve root sleeve. The dural nerve root sleeve is sensitive to pressure and produces pain in a segmental distribution. Cervical spinal nerves generally emerge horizontally and therefore the nerve roots are vulnerable to pressure only from the disc at that particular level, producing signs and symptoms in one segment only (Fig. 8.7). Indication of more than one nerve root involvement should be considered suspicious until proved otherwise.
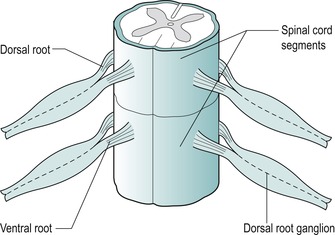 |
| Figure 8.7 Horizontal direction of emerging nerve roots. From Anatomy and Human Movement by Palastanga N, Field D and Soames R. Reprinted by permission of Elsevier Ltd. |
However, Tanaka et al (2000), in a cadaver study, showed that the roots below C5 reached their intervertebral foramen with increasing obliquity making compression of more than one nerve root below this level possible. At the C7–T1 disc, 78% of specimens showed that the C8 nerve roots did not have any contact with the disc at the entrance of the intervertebral foramen, which probably accounts for the low frequency of C8 radiculopathy.
Nerve root compression was found to occur at the en-trance of the intervertebral foramen and was determined to be due to herniated discs and osteophytes in the uncovertebral region anteriorly, and to the superior articular process, ligamentum flavum and periradicular fibrous tissue posteriorly (Tanaka et al 2000). Motor impairment, therefore, is suggestive of anterior compression from a disc prolapse or degenerative changes in the uncovertebral region, whereas sensory change is indicative of compression due to changes in the posterior structures. Of course a large disc prolapse or gross degenerative change, anteriorly or posteriorly, may compress both elements of the nerve root.
After it leaves the intervertebral foramen, the spinal nerve root immediately divides into ventral and dorsal rami. The sinuvertebral nerve is a mixed sensory and sympathetic nerve, receiving origin from the ventral ramus and the grey ramus communicans of the sympathetic system (Fig. 8.8). The nerve returns through the intervertebral foramen and gives off ascending, descending and transverse branches to supply structures at, above and below the segment (Oliver & Middleditch 2006, Palastanga et al 2006, Standring 2009). The structures it supplies include the dura mater, posterior longitudinal ligament and the outer part of the annulus of the intervertebral disc (Bogduk 1994b).
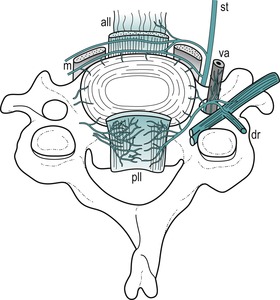 |
| Figure 8.8 A sketch of the innervation of the plexuses surrounding a cervical intervertebral disc (based on Groen et al 1990). The sinuvertebral nerves form a dense plexus accompanying the posterior longitudinal ligament (pll). Anteriorly, branches of the sympathetic trunk (st) supply the front of the disc and from a plexus accompanying the anterior longitudinal ligament (all). vr = ventral ramus, dr = dorsal ramus, va = vertebral artery, m = prevertebral muscles. From Grieve’s Modern Manual Therapy, 2nd edn by Boyling J D and Palastanga N. Reprinted by permission of Elsevier Ltd. |
Cervical arteries
Anatomically the vertebral artery is divided into the following four sections, which include two right-angled bends where it is vulnerable to internal and external factors which tend to compromise blood flow (Fig. 8.9) (Oliver & Middleditch 2006, Standring 2009):
• Its origin from the subclavian artery
• Its passage through each foramen transversarium except C7. In this section it gives off spinal branches which supply the spinal cord and its sheaths via the intervertebral foramen
• The first right-angled bend, turning medially to pass behind the lateral mass of the atlas
• The second right-angled bend, to turn vertically to enter the foramen magnum to unite with the other vertebral artery to form the basilar artery, which passes on to contribute to the circle of Willis.
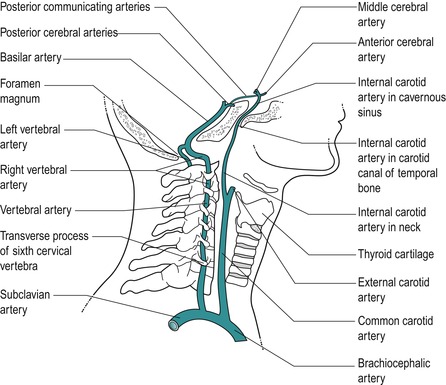 |
| Figure 8.9 Pathway of vertebrobasilar arteries. From Anatomy and Human Movement by Palastanga N, Field D and Soames R. Reprinted by permission of Elsevier Ltd. |
Anatomical anomalies and variations exist and commonly one vertebral artery is narrower than its partner. Clinically it is important to recognize vertebrobasilar signs and symptoms since these contraindicate certain cervical manoeuvres. The artery is elastic, particularly in its first and third sections, which allow it to accommodate to movement. Degenerative changes in the artery itself, in the intervertebral canal, uncovertebral joints and zygapophyseal joints make it vulnerable to blockage as well as possibly distorting its pathway.
The internal carotid artery arises from the bifurcation of the common carotid artery in the anterior cervical spine (Fig. 8.9). It supplies most of the ipsilateral cerebral hemisphere, the eye and accessory organs, the forehead and part of the nose. It ascends to enter the cranial cavity via the carotid canal and turns anteriorly to end by dividing into the anterior and middle cerebral arteries, which anastomose into the circle of Willis.
The internal carotid arteries together provide the most significant proportion of blood to the brain, 80%, compared with 20% passing through the posterior vertebral artery system. Blood flow is known to be influenced by neck movements, particularly extension and less so rotation (Rivett et al 1999, Kerry & Taylor 2006).
Differential diagnosis at the cervical spine
An understanding of the anatomy at the cervical spine, together with a detailed history and examination of the patient, will help with the selection of patients suitable for manual treatment and contribute to safe practice. The two areas of danger in this region are the cervical arteries and the spinal cord, and certain signs and symptoms will become evident on examination which would exclude some patients from manual treatment techniques.
Similarly, there are other causes of neck pain in which manual treatment techniques are either contra-indicated or not as appropriate. The following section will be divided into two parts. The first covers mechanical lesions, which present a set of signs and symptoms that help to establish diagnosis and to rationalize treatment programmes. The second covers the other causes of neck pain and associated signs and symptoms. On the whole, these patients are not appropriate for treatment with manual orthopaedic medicine treatment techniques and require suitable referral.
Mechanical cervical lesions
As well as being a primary source of pain, the disc, through prolapse into the vertebral or intervertebral canal, can have a secondary effect on any pain-sensitive structure lying within. This effect can be mechanical through compression and distortion, chemical through the inflammatory process and ischaemic through the pressure of oedema. For further information on these theories, the reader is referred to Chapter 13. Although the differences in the anatomy and function of the cervical and lumbar spine must be acknowledged, few studies have been unearthed to reflect patterns of radicular pain production specific to the cervical spine, although conclusions have been drawn in relation to myofascial pain patterns based on clinical observation. For the time being, cervical radicular pain patterns have been extrapolated from the lumbar model.
A central herniation of cervical disc material produces central and/or bilaterally referred symptoms. A unilateral herniation produces unilaterally referred symptoms. Reference of pain arising from compression of the central structures is characteristically multisegmental, i.e. over many segments (see Ch. 1). Involvement of the unilateral structures, dural nerve root sleeve and/or the nerve root produces segmentally referred signs and symptoms.
Since the disc degenerates early in the cervical spine, disc lesions tend to produce a pattern of symptoms which indicate a progression of the same condition. The symptoms are age-related with a pattern of increasing frequency and severity. Eventually the nerve root may become involved.
The anatomy of the zygapophyseal joint with its intra-articular structures makes it susceptible to possible mechanical derangement. It is difficult to differentiate pathology in the absence of neurological signs or symptoms, and primary disc lesions and zygapophyseal joint lesions appear to be similar in their presentation. Referral pain patterns arising from the zygapophyseal joints in symptomatic subjects have been looked at by Cooper et al (2007) who found that there was referral into the neck but minimal reference into the arm. As mentioned above, there are no similar studies for primary or secondary disc pain.
While acknowledging the zygapophyseal and other pain-sensitive somatic structures as possible causes of pain, the approach in orthopaedic medicine is traditionally based on the discal model.
Disc lesions in the cervical spine need to be reduced to prevent them contributing further to the degenerative process. A central prolapse in particular may cause osteophyte formation through ligamentous traction which may eventually threaten the spinal cord. Cyriax (1982) was emphatic in pointing out the danger of not reducing an early, minor cervical disc lesion for this reason as there comes a time when manipulation will not have an effect and a point at which it may be dangerous. Elderly patients with osteophytic cord compression often report the onset of paraesthesia associated with cervical extension and for that reason it would seem that particular attention should be paid to restoring cervical extension which would act as an indicator that reduction had been effected.
Cervical lesions produce a pattern of signs and symptoms and a set of clinical models has been established to aid diagnosis and establish treatment programmes. These are outlined later in this chapter. The models should be used as a general guide to the clinical diagnosis and treatment of cervical lesions. All show a non-capsular pattern on examination.
The following terminology will be used to describe disc lesions:
Disc protrusion
• Degenerate disc material bulges into the weakened laminate structure of the annulus, where it can produce primary disc pain since the outer annulus receives a nerve supply.
Disc prolapse
• Discal material passes through a ruptured annulus and/or posterior longitudinal ligament into the vertebral canal or intervertebral canal where it has a secondary effect on pain-sensitive structures: the posterior longitudinal ligament, dura mater, dural nerve root sleeve, nerve root and dorsal root ganglion. The sequela of this is sequestration of the disc.
Both forms of cervical disc lesion are suitable for orthopaedic medicine manual techniques, providing no contraindications exist.
Other causes of head and neck pain, arm pain and associated signs and symptoms
Generally, this group of conditions does not respond to the manual techniques described in this chapter and indeed some may be absolute contraindications. There may, however, be some overlap, particularly with the degenerative conditions, and the techniques may be attempted provided contraindications have been eliminated.
Arthritis in any joint presents with the capsular pattern. Arthritis occurs in synovial joints in the cervical spine and involves the zygapophyseal and uncovertebral joints. In the cervical spine the capsular pattern is demonstrated by the cervical spine as a whole. The limited movements have the ‘hard’ end-feel of arthritis. The pattern of symmetrical limitation of the side flexions and rotations is distinctive when compared with the asymmetrical pattern of limitation seen in disc lesions. The early degeneration of the cervical intervertebral disc occurs concurrently with degenerative changes within the other joints. The history will indicate the type of arthritis: degenerative osteoarthrosis, inflammatory or traumatic.
• Degenerative osteoarthrosis involves damage to hyaline cartilage and subchondral bone with sclerosis and osteophyte formation. Cervical movements become limited in the capsular pattern. Stiffening of the neck is particularly evident on rotation when the patient may, for example, have difficulty in reversing the car. Painful symptoms occur during acute exacerbations of the condition, precipitated by trauma or overuse.
The upper cervical segments are particularly involved in the degenerative process, with marked loss of rotation. Degenerative changes in the neck are often referred to as cervical spondylosis. However, despite gross X-ray changes, there may be little in the way of symptoms.
It is possible to have a disc lesion in an older degenerative neck, i.e. noncapsular pattern, superimposed onto a capsular pattern. The disc lesion can be treated with manual traction and the degenerative osteoarthrosis does not present a contraindication to treatment in itself. However, rotation under traction should be avoided due to the close proximity of the degenerate zygapophyseal and uncovertebral joints to the course of the vertebral artery (see below).
Degenerative changes in the uncovertebral joints lead to osteophyte formation which may encroach on the nerve root or adjacent vertebral arteries, causing problems through direct compression. Degenerative changes of the synovial joints may alter or distort the path of the vertebral artery, leading to possible compromise and symptoms.
• Matutinal headaches may be due to ligamentous contracture around the upper two cervical joints, the atlanto-occipital and atlantoaxial joints. A condition called ‘old man’s matutinal headache’ exists in which the patient, an elderly man, wakes every morning with a headache which usually eases after a few hours (Cyriax 1982). Mobilization techniques, particularly manual traction, may be appropriate for this condition.
• Tinnitus and vertigo may be associated symptoms of degenerative osteoarthrosis of the cervical spine. They can respond well to the techniques, but the vertebrobasilar system must be ruled out as a cause of the symptoms.
• Osteophytic root palsy produces a gradual onset of aching in the arm, usually with paraesthesia, as the osteophytes develop. The patient is usually elderly and will have objective neurological signs of weakness in the arm affecting one nerve root only. Since disc lesions presenting in this way are unusual in this age group, orthopaedic medicine techniques would be contraindicated.
• Cervical myelopathy may develop in association with degenerative changes in the cervical spine. Stenosis of the central canal occurs through osteophytic formation and hypertrophy and buckling of the ligamentum flavum develops. The osteophytes, a disc prolapse or a ligamentous fold may exert pressure on the spinal cord and a gradual onset of symptoms occurs with increasing disability. There may be pain, dysaesthesia of the hands consisting of numbness and tingling, clumsiness and weakness of the hands, weakness and evidence of spasticity of the lower limbs (Jenkins 1979, Connell & Wiesel 1992). The orthopaedic medicine treatment techniques described below would be contraindicated.
• Zygapophyseal joints could conceivably produce symptoms individually and in isolation to the other joints in the segment. As synovial joints they are prone to degenerative changes along with the other joints in the segment. Aprill et al (1989) suggested that distinct patterns of pain referral were associated with individual cervical zygapophyseal joints but others have refuted the existence of a facet syndrome (Schwarzer et al 1994).
• Cervical or cervicogenic headache describes a pain perceived to originate in the head but whose source is in the cervical spine (Bogduk 1992). It consists of an aching or deep pain localized to the neck, suboccipital and frontal region, precipitated or aggravated by neck movements or sustained neck postures, especially flexion. There is limitation of passive neck movements, changes in muscle contour, texture or tone and abnormal tenderness of the neck muscles (Sjaastad 1992, Beeton & Jull 1994, Jull (1994a) and Jull (1994b), Nilsson 1995, Schoensee et al 1995). The upper three cervical segments are most commonly involved and associated symptoms may consist of nausea, visual disturbances, dizziness or light-headedness (Jull (1994a) and Jull (1994b)).
Kerry & Taylor (2006) describe pain associated with carotid artery dissection that can present as ipsilateral posterior neck pain and/or frontotemporal headache. There are many forms of headache and the overlapping symptoms make it difficult to isolate headache due to primary cervical dysfunction. Orthopaedic medicine treatment techniques can be considered as an option if the carotid artery dysfunction and other contraindications have been ruled out.
• Polymyalgia rheumatica affects the middle and older age group, women more than men. It presents as pain and stiffness in the neck and shoulder girdle accompanied by fatigue, low-grade fever, depression and weight loss, and responds dramatically to small doses of oral corticosteroids (Hazelman 1995).
• Giant cell arteritis or temporal arteritis is a condition closely related to polymyalgia rheumatica. It is a vasculitis of unknown aetiology affecting the elderly. The patient presents with a severe temporal headache and scalp tenderness. The condition is treated urgently with high-dose steroids, to prevent blindness (Hazelman 1995).
• Rheumatoid arthritis is an inflammatory polyarthritis, affecting females more than males, with its onset usually between the ages of 40 and 50. It tends to follow a relapsing and remitting course. The synovial membrane becomes inflamed and thickened to become continuous with vascular tissue – a condition known as pannus. The pannus causes typical destructive changes of ligaments, cartilage and bone (Walker 1995). Rheumatoid arthritis can also involve extra-articular soft tissues, e.g. Achilles tendon, plantar fascia (Kumar & Clark 2002).
It is uncommon for rheumatoid arthritis to affect the cervical joints only, without its manifestation elsewhere, and it most commonly affects the smaller peripheral joints bilaterally. However, in patients with rheumatoid arthritis it may be silent in the cervical joints and there may be no clinical evidence of cervical spine involvement (Clark 1994).
The mechanism of the disease in the spinal joints is the same as that seen in peripheral joints, with ligament, cartilage and bone destruction. This loss of the supporting infrastructure of the spine, particularly of the upper cervical segment, is a potential hazard for significant neurological involvement of the brainstem and cervical spinal cord. Atlantoaxial subluxation is the most common manifestation, but cranial settling (vertical intrusion of the dens) and subaxial subluxation may also occur (Clark 1994, Zeidman & Ducker 1994, Mathews 1995). Rheumatoid arthritis is therefore an absolute contraindication to orthopaedic medicine techniques.
• Traumatic arthritis is produced by significant trauma causing inflammation in the cervical synovial joints and therefore a capsular pattern. This may occur following a whiplash injury. Once the capsular pattern has settled, there may be evidence of an underlying disc lesion to which mobilization can be carefully applied, providing there is no damage to the vertebrobasilar system.
• Whiplash injury occurs when a car is struck from behind, often while the occupants of the involved car are unaware. A hyperextension injury followed by a hyperflexion injury occurs. During the hyperextension phase the anterior structures, the intervertebral discs, anterior longitudinal ligament and anterior muscles can be damaged or torn and the posterior structures compressed. During the hyperflexion phase the dens may impact against the atlas, and the atlanto-occipital joint, posterior ligaments and zygapophyseal joints can be involved (Bogduk 1986). The alar and transverse ligaments and the tectorial and posterior atlanto-occipital membranes can be damaged by whiplash injury (Krakenes et al 2002, Krakenes et al 2003). Generally, a whiplash injury may produce some pain initially, but it is not until later that the ligaments stiffen and produce a secondary capsular pattern due to the trauma.
Significant bony or ligamentous damage causes immediate pain with a reluctance to move the neck. X-ray evidence of cervical instability is an absolute contraindication to orthopaedic medicine techniques. A history of recent whiplash injury has been identified as a possible risk factor of vascular accident (Kleynhans & Terrett 1985).
Taylor & Twomey (1993) conducted an autopsy study of neck sprains and showed clefts associated with vertebral end-plate lesions in trauma victims. These were distinct from the uncovertebral clefts and central fissures associated with degeneration of cervical discs. These so-called rim lesions involved the avascular cartilage end-plates and the outer annulus and, in further experiments, showed a poor response to healing. They may be responsible for the chronic pain often associated with whiplash injuries. Posterior disc herniation through a damaged annulus and haemarthrosis of the zygapophyseal joints were also observed in the trauma victims and this is clinically significant in treating the early whiplash. The acute sprain of the joints makes this an irritable lesion which requires pain relief and reduction of inflammation. Early mobilization – in line with the principles for acute lesions laid out in Chapter 4– may be applied, providing gross bony injury and instability are not present.
Evidence exists to support early mobilization in whiplash-type injuries to avoid the chronic pain syndrome developing, with its associated psychosocial factors (Mealy et al 1986, McKinney 1989). Current literature suggests that at 3 months, approximately one-third of subjects with whiplash injury will have high levels of persisting pain and disability (Stewart et al 2007). The Chartered Society of Physiotherapy has produced guidelines for the management of whiplash associated disorder (WAD) following a review of the available evidence (Moore et al 2005). The guidelines aim to support practice and to help both physiotherapists and patients to make informed choices for continuing management following assessment.
The recommendations are summarized as follows:
• In the acute stage (0–2 weeks after injury) patients should be given education, active exercise, and advice on self-management and a return to normal activity as soon as possible.
• In the subacute stage (2–12 weeks after injury) a multimodal approach should be applied including postural training, manual techniques and psychological support. There is evidence to support that combined manipulation and mobilization, muscle retraining including deep flexor activity, acupuncture, education, advice on coping strategies, TENS (transcutaneous electrical nerve stimulation), massage and soft tissue techniques may contribute to pain reduction.
• In the chronic stage (more than 12 weeks after injury) exercise therapy, manipulation and mobilization (which may be combined) and multidisciplinary psychosocial packages may be effective. Trained health professionals (who are not necessarily psychologists) can give psychological support.
Within the orthopaedic medicine approach, gentle techniques have been devised for pain relief and return of function in the acute stage, i.e. at an earlier stage than that recommended by the guidelines. Two randomized controlled trials relating to manual mobilization techniques were scrutinized in the guidelines and both were found to have flaws.
The conclusion was that there is no evidence regarding the short- or long-term benefit of early mobilization, However, Taylor & Kerry (2005) cite Cassidy et al (1992) and Baltaci et al (2001) to support the ‘commonly held view’ that mechanical pain of acute onset responds well to early manipulation, although pain arising from whiplash injury is not specified. There does not appear to be evidence of no benefit.
Sterling & Kenardy (2008) looked at the heterogeneity of whiplash and observe that it is inappropriate to apply the same programmes of management to all individuals since they display a wide range of different characteristics and responses following the injury. They recommend that more research needs to be done to be able to identify features of the condition that may be identifiable at early assessment, particularly as predictors of poor recovery, to allow for more specific treatment directions.
The techniques suggested below include Grade A mobilization, providing there is no serious pathology. In accordance with the guidelines, the patient is given the responsibility for self-management of the condition, and is instructed about posture and exercise, advice to avoid excessive reliance on a collar, appropriate pillow support and adequate analgesia.
Serious, non-mechanical conditions may present with signs and symptoms similar to those of a mechanical presentation. For this reason, careful examination is necessary to eliminate serious disease which would be contraindicated for orthopaedic medicine treatment. Patients may present with local symptoms which are rarely provoked by movement or posture. On examination it may be difficult to reproduce the symptoms. Other more generalized features may also be present, such as increasing and unrelenting pain, night pain, weight loss, general malaise, fever, raised erythrocyte sedimentation rate or other symptoms, e.g. cough.
• Spinal infections may include osteomyelitis or epidural abscess. The organism responsible may be Staphylococcus aureus, Mycobacterium tuberculosis or, rarely, Brucella (Kumar & Clark 2002).
• Malignant disease is usually extradural with bone metastases produced most commonly from primaries in the bronchus, breast, prostate, kidney or thyroid. There may be a history of a gradual onset of pain and stiffness, the pain tends to be unrelenting and night pain is usually a feature. The pain is not relieved by different postures. On examination active movements produce pain and limitation in all directions. The passive movements are prevented by the end-feel of a twang of muscle spasm and resisted movements are painful and possibly weak. All of these signs and symp-toms are evidence of a gross lesion (Cyriax 1982). Neurological examination may reveal excessive muscle weakness involving several nerve roots, possibly bilaterally, in contrast to a disc lesion that tends to involve one nerve root only (Mathews 1995).
• Primary tumours (e.g. meningioma, neurofibroma, glioma) tend to present with a gradual onset of symptoms of cord compression and pain is not usually a major feature.
• Pancoast’s tumour is carcinoma in the apex of the lung which may erode the ribs and involve the lower brachial plexus. It accounts for only 5% of bronchial tumours. There is severe pain in the shoulder and down the medial aspect of the arm, with evidence of C8 and/or T1 palsy, possible atrophy of the ulnar aspect of the hand and a reduced triceps reflex (Pitz et al 2004). Cervical side flexion away from the painful side may be the only limited neck movement, with passive elevation of the shoulder on the symptomatic side also being painful (Cyriax 1982). Interruption of the sympathetic ganglia can produce Horner’s syndrome – constriction of the pupil and drooping of the eyelid on the side of the tumour (Kumar & Clark 2002).
The following conditions are not serious but should be considered as part of the clinical reasoning required in differential diagnosis:
• Suprascapular, long thoracic and spinal accessory neuritis usually present with pain in the scapula and upper arm of approximately 3 weeks’ duration. On examination, the neck movements are full and do not reproduce the pain. There is weakness of the appropriate muscles supplied by the affected nerve. The cause may be unknown, or it may be due to trauma or follow a viral infection. Recovery is usually spontaneous over approximately 6 weeks.
■ Suprascapular neuritis produces weakness of the supraspinatus and infraspinatus muscles
■ Long thoracic neuritis produces weakness of the serratus anterior muscle and winging of the scapula
■ Spinal accessory neuritis produces weakness of the sternocleidomastoid and trapezius muscles
• Neuralgic amyotrophy is an unusual cause of severe pain in the neck and scapular region with a bizarre pattern of muscle weakness in the infraspinatus, supraspinatus, deltoid, triceps and serratus anterior muscles. The cause of the condition is unknown, but it may follow viral infection or immunization and an allergic basis is postulated (Kumar & Clark 2002). It usually recovers spontaneously over several weeks or months, although recovery may be more prolonged in some cases.
• The pain of shingles (herpes zoster) can precede the rash and cervical pain and headache have been reported prior to the appearance of vesicles in the cervical region.
Thoracic outlet syndrome, reflex sympathetic dystrophy and work-related syndromes all present with upper limb signs and symptoms which are sometimes difficult to isolate into a simple diagnostic pattern, particularly if symptoms have been present for a long time.
■ Thoracic outlet syndrome is a term used for compression, entrapment and/or postural alterations affecting the brachial plexus and its accompanying neurovascular structures, although debate continues about its existence (Walsh 1994). Distal symptoms occur, usually due to compression of the lower trunk of the brachial plexus (C8, T1), but the upper and middle trunks can also be involved. The condition may be bilateral, with a burning, dull aching pain along the medial aspect of the forearm. Distal oedema may be associated with activity, sweating and heaviness, and circulatory changes may be seen in the hands. Paraesthesia occurs as the release phenomenon, coming on at night, some time after the pressure has been released.
■ Reflex sympathetic dystrophy describes a complex disorder of the limbs with or without obvious nerve involvement. It consists of persistent peripheral burning pain and tenderness which is termed hyperaesthesia (an abnormal response to pain) or allodynia (pain in response to stimuli that are not normally noxious). Vasomotor and sensory changes consist of sweating, colour changes and trophic skin changes together with weakness, tremor, muscle spasm and contractures (Herrick 1995).
■ Work-related syndromes of the upper limb are due to repetitive occupational overuse, producing musculoskeletal symptoms, once a certain threshold of activity is exceeded. Sometimes this may present as a simple tenosynovitis or tendinopathy but much more often it presents as a catalogue of symptoms which are non-specific. Diffuse aching, stiffness, muscle or joint tiredness are present with the chronic nature of the condition, perhaps leading to anxiety and depression (Bird 1995). The symptoms here are usually associated with factors that affect the vmobility and circulation of the nervous system. Each component needs to be recognized and a suitable treatment programme established. Neural tensioning techniques can be applied to assess neural mobility which can be addressed as part of treatment and self-management. Orthopaedic medicine techniques are not usually indicated unless specific identifiable lesions are diagnosed.
• Fibromyalgia usually presents in women, as a complex of variable symptoms including widespread musculoskeletal pain of the neck, shoulders and upper limbs. Fatigue, headache, waking unrefreshed, subjective distal swelling, poor concentration, forgetfulness and weepiness have been described (Doherty 1995). Multiple hyperalgesic tender spots and non-restorative sleep are the main diagnostic features of fibromyalgia. There are several components to management: they include the use of relaxation techniques, exercise, hydrotherapy, physiotherapy, acupuncture, muscle relaxants and drugs to improve the quality of sleep. The condition is difficult to separate from endo-genous depression and often responds to antidepressant medication (E. Huskisson, conference note 1995).
• Cervical spine instability is controversial and difficult to diagnose, and there do not appear to be valid or reliable tests to help with diagnosis (Cook et al 2005). Instability may contribute to the clinical presentation of various conditions including cervicogenic headache, chronic whiplash associated disorder, rheumatoid arthritis, osteoarthritis and segmental degeneration. Trauma, genetic predisposition (e.g Down’s syndrome), disc degeneration and surgery may compromise the stabilizing mechanisms of the spine (Cook et al 2005).
In some cases the instability can be potentially life threatening as in laxity of the transverse ligament associated with rheumatoid arthritis or Down’s syndrome where the odontoid peg may be hypoplasic or deformed. Subluxation of the atlantoaxial joint and hypermobility of the atlanto-occipital joint are associated with Down’s syndrome and may occasionally lead to compression of the spinal cord. Clinicians involved in manipulation should be aware of this risk (Pueschel et al 1992, Department of Health 1995, Matsuda et al 1995).
Upper cervical instability has been associated with localized atherosclerotic changes in the cervical vessels. The changes may be associated with repeated microtrauma as a result of increased upper cervical movement. This can be associated with connective tissue inflammatory disease, principally rheumatoid arthritis, or acute whiplash injury, as mentioned above (Kerry & Taylor 2006).
• Drop attacks are sudden episodes of weakness in the lower limbs, causing falling without loss of consciousness and complete recovery in seconds or minutes. Drop attacks are a symptom, not a diagnosis, and they can have diverse causes. They may be due to changes in tone in the lower limb originating in the brainstem, and appear to be related to transient ischaemic attacks (Kumar & Clark 2002). Any instability in the upper cervical segment – i.e. congenital ligamentous laxity of the atlanto-occipital joint, deformed odontoid process, cervical spondylosis or a spondylolisthesis – can produce drop attacks (Cyriax 1982, Hinton et al 1993).
They may also be due to the heart (a variant of syncope) or problems with both the heart and circulation to the brain. Seizures and Ménière’s disease can be associated with drop attacks and other rare causes have been reported (Hain 2009). During the subjective examination the patient must be questioned about drop attacks and the result noted. Any history of drop attacks is an absolute contraindication to orthopaedic medicine treatment techniques.
• Klippel–Feil syndrome is associated with a limited range of cervical movement, short neck and low hairline. Patients usually have developmental abnormalities, including congenital fusion of cervical vertebrae, which may predispose them to the risk of neurological sequelae (Pizzutillo et al 1994).
Cervical artery dysfunction
• Vertebrobasilar insufficiency produces symptoms through a reduced blood flow in the vertebral arteries to the hind brain. Patients often relate their symptoms to particular head positions such as looking up (Toole & Tucker 1960). Anatomical anomalies are frequently seen in the vertebral arteries and their course through the cervical foramen transversarium. Often the two arteries vary considerably in diameter (Mitchell & McKay 1995) and extrinsic or intrinsic factors may decrease the lumen of the artery permanently or temporarily. Extrinsic factors include degenerative changes in the intervertebral, zygapophyseal and uncovertebral joints, with osteophyte formation, which may compress or alter the course of the artery. Intrinsic factors include arterial disease and thrombosis.
Wallenberg’s syndrome or lateral medullary syndrome is probably the most recognized syndrome of brainstem infarction caused by vertebral artery pathology (Frumkin & Baloh 1990, Kumar & Clark 2002). The common site of injury to the vertebral artery following neck manipulation is at the level of the atlantoaxial joint. Injuries include intimal tearing, dissection or thrombus formation, intramural haematoma or vasospasm.
Dizziness and nausea are the main presenting symptoms of vertebrobasilar insufficiency. However, such symptoms are also associated with cervical dysfunction; therefore correct diagnosis is important. A full list of possible signs and symptoms of vertebrobasilar insufficiency is given with the description of the test later in this chapter.
• Carotid artery dissection can present suddenly and may arise from a sudden movement of the neck involving extension and rotation (Taylor & Kerry 2005). It typically presents with unilateral upper cervical or anterolateral neck pain with headache and/or sensitivity in the frontotemporal region (Kerry & Taylor 2006). Horner’s syndrome may be present, associated with ptosis (drooping eyelid), sunken eye, a small constricted pupil and facial dryness. Symptoms of vertebrobasilar artery insuffiency (VBI) may also be present.
• Young: Under 20
• Elderly: First episode over 55
• VBI/CAD symptoms
• Previous whiplash/trauma
• Past medical history of malignancy
• Constant progressive pain
• Unremitting night pain
• Systemically unwell
• Unexplained weight loss
• Drug abuse and HIV
• Long-term systemic steroid use
• Cough/sneeze increasing arm pain
• Pain gradually worsening over 3 months
• Neurological signs and symptoms affecting more than one nerve root
• Inflammatory arthritis
• Osteopoenic/osteoporotic
• Down’s syndrome
• Arm pain under 35
• Side flexion away being only painful cervical movement
• T1 weakness
• Horner’s syndrome
• Upper motor neurone signs
• Risk factors for atherosclerosis
COMMENTARY ON THE EXAMINATION
Observation
Before proceeding with the history, a general observation of the patient’s face, posture and gait is made, noting the posture of the neck and the carriage of the head. Neck posture will give an immediate indication of the severity and possible irritability of the condition, e.g. a wry neck associated with acute pain in which the patient has developed an antalgic posture.
The box above lists the ‘red flags’ for the possible presence of serious pathology that should be listened for and identified throughout the subjective and objective examination. In isolation, many of the flags may have limited significance but it is for the clinician to consider the general profile of the patient and to decide whether contraindications to treatment exist and/or whether onward referral is indicated.
History (subjective examination)
The history is particularly important at the spinal joints. Selection of patients for orthopaedic medicine treatment techniques relies on the discal model of diagnosis and certain aspects of the history will assist in this diagnosis as well as highlighting patients with contraindications to treatment.
The age, occupation, sports, hobbies and lifestyle of the patient may give an indication of the nature of onset and its relationship to habitual postural problems associated with a particular lifestyle.
The age of the patient is important, particularly at the cervical spine, since the type of cervical disc lesion is related to age. In the young patient, child or adolescent, neck pain may be associated with an acute torticollis, possibly a true nuclear disc lesion.
Disc lesions tend to occur in the middle-age group, with posterior or posterolateral herniation; zygaphophyseal joint lesions are also prevalent in this age group. Referred arm pain, due to a large posterolateral disc prolapse, usually occurs over the age of 35, through progressive prolapse. Arm pain presenting under the age of 35 may be indicative of serious pathology and this should be excluded. Degenerative changes in the intervertebral, uncovertebral and zygapophyseal joints occur in the older neck.
Occupation, sports, hobbies and lifestyle of the patient may contribute to the patient’s signs and symptoms. Habitual postures can contribute to postural adjustment, altered biomechanics and muscle imbalance. Examples are provided by the head-forward posture of the visual display unit operator, the side-flexed posture of holding the telephone in the crook of the neck to leave the hands free, the flexed and rotated posture of the plumber or builder, or the head-extended posture allowing the arms to be used above the head in the painter or electrician. Athletes may assume certain postures related to their sport which may precipitate or contribute to their problem.
The site and spread of the symptoms give important clues to diagnosis in the cervical spine and highlight the importance of understanding the mechanisms of referred pain in a segmental or multisegmental pattern. Pain may be localized to the neck or occur in association with symptoms felt in the scapular area, chest, upper limb or head. The sole presentation of internal carotid artery dysfunction may be unilateral upper cervical or anterolateral neck pain and headache and/or sensitivity in the frontotemporal region (Kerry & Taylor 2006).
Nerve root compression in the cervical spine can only occur at the levels at which the nerve root can be compressed. In the mid and lower cervical regions the roots are under threat from the intervertebral discs, uncovertebral joints and zygapophyseal joints which form the boundaries of the intervertebral foramen. C1 and 2 nerve roots do not run in intervertebral foramina, therefore compression of these nerve roots is not the mechanism for upper cervical pain.
It is important to establish the nature of the onset and duration of the symptoms, not just of this current episode of pain, but of all previous episodes. Cervical disc lesions tend to be a progression of the same incident, and establishing a history of increasing and worsening episodes of pain assists diagnosis.
The onset may be sudden or gradual. It may be precipitated by a single incident, such as a whiplash injury due to a motor vehicle accident, or a sudden unguarded movement, such as missing a footing. If traumatic in onset, the exact mechanism should be established: was it hyperflexion, hyperextension or excessive rotation? If the condition developed gradually, is it associated with habitual postures, or a change in posture, such as sleeping in a different bed?
The patient with whiplash injury without serious bony complications presents with pain felt at the time of the trauma which settles. Twenty-four hours later, pain and stiffness develop due to the ligamentous involvement and muscular strain. The whiplash patient who has severe pain from the time of the trauma may have more serious underlying pathology, e.g. fracture and/or dislocation.
Headache of sudden onset may be an indication of internal carotid artery dysfunction (Taylor & Kerry 2005, Kerry & Taylor 2006).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


