Chapter 14 The Arthritides
Disorders of the joints are common and may cause considerable pain and disability. They are frequently classified as noninflammatory, inflammatory, or infectious. This chapter reviews the more common joint affections.
The Synovium
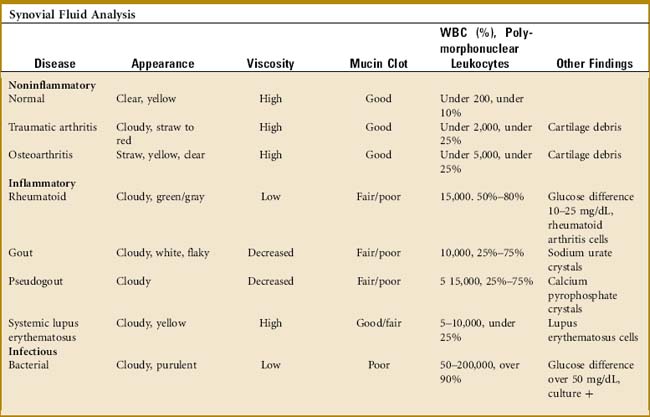
A great deal of information can be obtained from the examination of a joint aspirate (Table 14-1). However, this examination is not indicated in every joint effusion and should be limited to those diagnostic problems that are not secondary to trauma. (Usually, the two disorders of most concern are infection and crystalline arthritis.) The joint is usually aspirated from the extensor side under sterile conditions. Three test tubes are sufficient for most determinations: (1) a plain tube for gross examination, clotting, and a mucin clot test; (2) one ethylenediaminetetraacetic acid–treated tube for cell and crystal analysis; and (3) one heparinized tube for bacteriologic study. Five milliliters of fluid are placed in each tube.
THE MUCIN CLOT TEST
This test determines the amount of hyaluronate in the fluid. Acetic acid is added to the tube, and the sample is observed for clot formation. A “poor” mucin clot indicates a decrease in hyaluronate. This results from dilution, depolymerization, and loss of filter function from either inflammation or infection. A “good” clot is present in normal fluid and osteoarthritis.
Osteoarthritis
CLINICAL FEATURES
Pain is the most common initial symptom. This frequently occurs with motion or activity and is relieved by rest. The source of discomfort is unknown. It may result from chemical mediators and possibly mechanical factors. Joint stiffness typically occurs with rest and improves with activity. The physical findings include crepitus, joint line tenderness, swelling, restriction of motion, and joint enlargement from osteophyte formation. In the hands, these osteophytic overgrowths are termed Heberden’s nodes when they are present at the distal interphalangeal joint and Bouchard’s nodes when they occur at the proximal interphalangeal joint. Pain is usually present on joint motion. Disuse atrophy of the adjacent musculature may develop rapidly, thus increasing the disability and pain. Even though osteoarthritis is not considered an “inflammatory” disease, mild increased temperature with palpable heat is often present. This can be appreciated clinically in a superficial joint (such as the knee) by placing one hand on the front of each knee of the sitting patient and then switching the hands back and forth. Subtle differences in temperature suggestive of synovitis (which indicates an intraarticular problem) may become more apparent. This clinical test is often helpful in the obese patient in whom an effusion may be difficult to visualize.
The roentgenographic findings consist of joint space narrowing, spur formation, sclerosis, and subchondral cyst formation (Fig. 14-1). The laboratory findings and synovial analysis are normal, except for occasional flakes of cartilage in the joint fluid. In most cases, a routine physical examination and plain films are sufficient to establish the diagnosis. More extensive radiographic testing is usually not indicated except in those cases in which the diagnosis is uncertain.

TREATMENT
Stretching exercises are helpful, and the joint should be passed through a full range of motion several times daily to reduce joint stiffness. The local application of moist heat often relieves discomfort during the acute painful stage and may be especially helpful before exercise. Exercises designed to combat stiffness and restore muscle strength are important, because the weakness contributes to joint instability and disability. The patient may benefit from a short course of formal physical therapy to develop a good home exercise program. All exercise should be low impact. Aquatic exercise programs are generally well tolerated. Nonsteroidal anti-inflammatory drugs (NSAIDs) are traditionally used for osteoarthritis, but may be no more effective than acetominophen for pain relief because the role of inflammation in the condition is uncertain. Mild analgesics may even be indicated on an occasional basis. Intraarticular cortisone injections are often very effective for pain relief. Their effect is usually only temporary, but the benefit may last several months. The injections can be repeated several times per year. Any recommended limits to the number of injections a patient may have per year appears to be arbitrary, although most patients seem to do well with three or four injections per year. Various liniments may be used for their counterirritant effect. Viscosupplementation (a series of joint injections using a hyaluronate-like material) has been tried, but the results are inconclusive. The efficacy of supplements such as chondroitin and glucosamine has not been well proven.
Orthopedic referral is indicated when there is no response to medical management. The most common surgical procedures are arthrodesis and arthroplasty (Fig. 14-2). Each is effective in eliminating the painful articulation. Realignment of faulty weight-bearing joints by osteotomy may also be beneficial.

GOUT
CLINICAL FEATURES
The initial acute attack is usually of sudden onset and occurs in a single joint or area of tenosynovium of the lower extremity (Table 14-2). The metatarsophalangeal (MTP) joint of the great toe is classically the first site of involvement (podagra), although any joint or area of tenosynovium can be involved. The extensor synovium on the dorsum of the midfoot is another common site of acute attack, as is the knee joint (gonagra). In 80% to 90% of cases, the lower extremity is involved. The older patient with gout is more likely to have involvement of the fingers and to develop tophi. Older women may present with polyarticular disease, often involving atypical locations. The pain and inflammation are usually severe and may be precipitated by exercise, dietary indiscretion, and physical or emotional stress. Attacks are common after illness or shortly after surgery, and they typically begin at night. Swelling, heat, redness, and other signs of inflammation are usually present. The physical findings may even simulate cellulitis or infectious arthritis. The area is often tender to even the slightest touch. Fever, tachycardia, and other constitutional symptoms may accompany the attack. The initial episode may be followed later by polyarticular involvement. Eventually, deposits of urate crystals, termed tophi, may form in the subcutaneous tissue.
Table 14-2 Joint Swelling—Differential Diagnosis*
| Disorder | Symptoms/History | Findings |
|---|---|---|
| Pyogenic arthritis | Usually painful but sometimes low grade. Fever, acute onset. Usually monoarticular. | Febrile, increased heat, painful movement. Systemic signs of illness. Joint fluid positive for bacteria. |
| Gouty arthritis | Knee, great toe, or generalized foot pain. Symptoms may be initiated by physical stress such as surgery. May be extremely painful but usually low grade. Usually monoarticular. Previous episodes? | Redness, increased heat. Crystals in joint fluid. Elevated serum uric acid. Fluid often cloudy. |
| Osteoarthritis | Chronic, gradual. Monoarticular. May have history of mechanical injury. Stiffness after rest, pain after prolonged activity | Restricted movement but pain usually only at the extremes of movement. Fluid is clear, only excessive amounts. |
| Pseudogout | Middle age to elderly. Usually monoarticular. Previous episodes? | Crystals in cloudy fluid (calcium pyrophosphate). |
| Rheumatoid arthritis | Multiple joints may be involved. Females most commonly affected. Usually subacute or insidous in onset but occasionally acute. Often symmetric. Metacarpophalangeal, proximal interphalangeal joints usually involved. | Subcutaneous nodules in late cases. Laboratory studies may show positive rheumatoid test and increased ESR. |
| Others | History may reflect skin rash or other skin changes. Note other system involvement (complete history, especially GI, and pulmonary system). | FANA, ESR may be abnormal. Many collagen disorders have polyarticular symptoms and act like rheumatoid arthritis. |
ESR, Erythrocyte sedimentation rate; FANA, flurorescent antinuclear antibody; GI, gastrointestinal.
* NOTES: The workup should include aspiration of joint fluid. Fluid is observed for color, and the string test is performed. The fluid is analyzed for cell count, Gram stain, crystal analysis, and culture and sensitivity. The blood work should include complete blood cell count, uric acid, blood cultures if indicated, sedimentation rate, fluorescent antinuclear antibody, and rheumatoid factor. Blood cultures should include aerobic and anaerobic cultures. Roentgenographic evaluation is always performed to evaluate for osteoarthritis and calcific changes in soft tissues.
Early in the disease, roentgenogram findings are normal. Later, erosive changes appear that have a characteristic punched-out appearance (Fig. 14-3). Destruction and degeneration of the articular cartilage frequently follow.

The standard for the definitive diagnosis of gout requires crystal identification on joint aspirate, although a presumptive diagnosis is often established on clinical grounds, especially if associated with hyperuricemia. Laboratory findings include a mild leukocytosis, elevated sedimentation rate, and hyperuricemia, although acute attacks are occasionally associated with a normal level of uric acid. In some patients, the SUA level may decrease into the normal range during an acute attack. Uric acid levels are best checked again after the attack is over. The synovial aspirate is usually cloudy and mildly inflammatory in nature. Because acute gout and infectious arthritis can present identically, the fluid should also be tested for infection. Urate crystals are usually demonstrable. They are needle shaped and negatively birefringent (shine brightly) under polarized light. A 24-hour urinary collection for uric acid may be helpful in determining the appropriate treatment.
TREATMENT
The treatment of gout depends on the stage of the disease. The objectives in management are to terminate or prevent the acute attack, encourage mobilization of tophaceous deposits, and reduce the level of SUA.
Surgery is usually limited to excision of large tophi and, occasionally, arthroplasty.
Pseudogout (Chondrocalcinosis)
CLINICAL FEATURES
The clinical presentation is variable, but the symptoms are similar to those of chronic gouty arthritis. The age of onset is 60 to 70 years. Intermittent acute episodes occur, but the joint most commonly involved is the knee rather than the great toe. The attacks are usually monoarticular. The condition is frequently familial and is occasionally associated with diabetes, renal disease, and other systemic conditions. Like gout, acute attacks may be triggered by a variety of surgical or medical events. In addition to the goutlike symptoms, calcification of the cartilage of the knee, especially the meniscus, is common (Fig. 14-4). Calcification of the anulus fibrosus, radioulnar disc, and symphysis pubis may also be seen. Stippled calcification in bands running parallel to the subchondral bone margins may be present. Synovial fluid analysis reveals typical rhomboid-shape crystals that exhibit weakly positive birefringence under polarized light. There are no specific changes in blood or urine. The American Rheumatism Association criteria are often used for diagnosis:

Rheumatoid Arthritis
The etiology of the disorder is unknown, although it is most likely an immune response to some antigen, possibly viral. The result is the activation, by some unknown mechanism, of proinflammatory cells that infiltrate the synovium. These cells, in turn, release various substances such as cytokines and tumor necrosis factor (TNF)-α, which subsequently cause the pathologic changes typical to this group of diseases. Pathologically, the synovium becomes thickened, inflamed, and hypertrophic. An aggressive, infiltrating granulation tissue from the synovium (pannus) typically spreads over the joint cartilage. Eventually, erosion and destruction of the articular surface result from the chronic inflammatory process.
CLINICAL FEATURES
The onset is usually gradual although acute cases may occur. Weakness, fatigue, and anorexia are common prodromal symptoms. Eventually, joint involvement becomes apparent, with stiffness, swelling, heat, and redness. Stiffness is most pronounced in the morning because of the “gelling” effect of the excess fluid. Most cases initially present with multiple symmetric joint involvement, most often in the hands and feet (Table 14-3). The MCP, metatarsophalangeal (MTP), and proximal interphalangeal (PIP) joints are usually involved, but the distal interphalangeal (DIP) joints are not. Eventually, most of the major joints become involved as well. Remissions and exacerbations are common, but the condition is chronically progressive in the majority of cases. The disease shortens life expectancy from 10 to 15 years.
Table 14-3 American Rheumatology Revised Classification of Rheumatoid Arthritis (American College of Rheumatology)
| Rheumatoid arthritis is said to exist when four of the following seven conditions are present: |
| (Criteria 1–4 must be present for at least 6 weeks.) |
The roentgenogram usually reveals soft tissue swelling and osteoporosis early in the disease. Eventually, joint space narrowing, erosion, and deformity become visible as the result of continued inflammation and cartilage destruction (Fig. 14-5).







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


