6 The Arthritic Lower Extremity
The arthritic hip
Pathology around the hip can be classified into three groups: intra-articular, extra-articular, and hip mimickers (Table 6-1).
Table 6-1 Potential Causes of Groin Pain in Athletes
| Intra-Articular | Extra-Articular | Hip Mimickers |
|---|---|---|
| Acetabular labral tears Ligamentum teres tears Femoroacetabular impingement Chondral defects Osteoarthritis Avascular necrosis Dysplasia | Internal coxa saltans External coxa saltans Gluteal tears Muscle strains Piriformis syndrome Slipped capital femoral epiphysis Fractures | Athletic pubalgia (sports hernia) Osteitis pubis Genitourinary disorders Intra-abdominal disorders Lumbar radiculopathy |
General Features of Osteoarthritis
According to Dieppe (1984), the following are general features of osteoarthritis:
Diagnosis of Hip Arthritis
The American College of Rheumatology lists several criteria for the diagnosis of OA of the hip.
Treatment of Hip Arthritis
Nonoperative Treatment
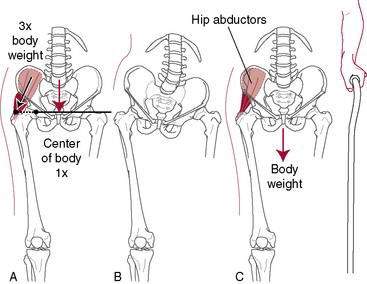
A cane in the opposite hand helps to unload the hip significantly (Fig. 6-1). A properly fitted cane should reach the top of the greater trochanter of the patient’s hip while wearing shoes. Doing stretching and strengthening exercises or joining a yoga class can be of surprising value in terms of regaining ROM because it is not uncommon that stiffness of periarticular structures (e.g., the inability to put on shoes and socks) rather than pain makes surgery necessary.
Medical Treatment
Acetaminophen is the most commonly used oral medication for OA. In addition to its anti-inflammatory effect, acetaminophen acts as an inhibitor of cyclo-oxygenase (COX)-1 and COX-2 in the central nervous system. Several clinical guidelines for the treatment of OA recommend its use for the relief of mild to moderate OA pain (American College of Rheumatology [www.rheumatology.org], Osteoarthritis Research Society International [www.oarsi.org], European League Against Rheumatism [www.eular.org]). A 2006 Cochrane review (Towheed et al.), however, found that although acetaminophen was significantly superior to placebo for pain relief, the clinical significance of the improvement was dubious. Although acetaminophen is among the safest oral analgesics, it does carry some risk for hepatic toxicity, although rarely at doses of 4 g/day or less.
Neutraceuticals such as glucosamine and chondroitin sulfate are popular but unproven. Glucosamine and chondroitin sulfate are synergistic endogenous molecules in articular cartilage. Glucosamine is thought to stimulate chondrocyte and synoviocyte metabolism, and chondroitin sulfate is believed to inhibit degradative enzymes and prevent formation of fibrin thrombi in periarticular tissues (Ghosh et al. 1992).
Injections of steroids can provide temporary relief but are not of lasting benefit and should not be done too frequently because of the risk of side effects such as weakening of the soft tissues around the hip joint and possibly the bone itself. More recently, hyaluronate injections have been reported to be effective in some patients (Migliore et al. 2009), whereas other have reported no benefit (Richette et al. 2009). This treatment currently is investigational for hip arthritis and is considered an “off-label” use.
Operative Options for Hip Arthritis
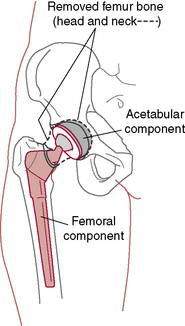
Osteotomies, such as pelvic and intertrochanteric osteotomies, were popular in the past, and they still may have a limited role in selected situations. Fusion still does have a role but in very early childhood only. The mainstay of surgical treatment is total hip replacement (Fig. 6-2). In general, for elderly patients with low activity demands, both the acetabular and the stem components can be cemented. For patients who are young and high demand, the current trend is to use noncemented implants. These are only general guidelines. In revisions with poor-quality bone, the surgeon makes fixation choices based on intraoperative findings.
Total Hip Replacement Rehabilitation: Progression and Restrictions
Morteza Meftah, MD; Amar S. Ranawat, MD; and Anil S. Ranawat, MD
The success of total hip replacement (THR) is a result of predictable pain relief, improvements in quality of life, and restoration of normal function (Brown et al. 2009). Postoperative rehabilitation is one of the factors that can affect outcomes after THR. The main goal of postoperative rehabilitation protocols is achieving maximal functional performance by focusing on reducing pain, increasing ROM, and strengthening the hip muscles (Brander et al. 1994) (see also page 435).
Because the majority of functional performance is gained within the first 6 months postoperatively (Gogia et al. 1994), a proper rehabilitation program that addresses the aforementioned goal is of paramount importance. Several factors influence the results of these programs, such as preoperative management, surgical approach, multimodal pain control modalities, hip precautions, postoperative protocols, weightbearing status, and the level of rehabilitative care.
Preoperative Management
Patient education regarding postoperative pain management, restrictions, independent walking, and proper rehabilitation is an important first step in achieving satisfactory results after THR. Preoperative classes can facilitate patients’ understanding of reasonable expectations of recovery, increase their motivation, and help expedite the rehabilitation learning process(Giraduet-Le Quintrec et al. 2003). Vukomanovic et al. reported that patients who both performed the “postoperative” exercises and received preoperative education demonstrated the ability to perform functional activities significantly earlier than those who were randomly assigned to the control group. These functional activities included being able to walk up and down stairs earlier, use the toilet and chair sooner, transfer independently, and ambulate independently.
Patient education also has been shown to be directly related to faster postoperative ambulation, reductions in hospital length of stay, and less use of narcotic pain medications (Spaulding 1995). A major part of preoperative educational classes should be dedicated to prevention of postoperative dislocation by appropriate explanation of hip precautions.
Although several studies have shown that preoperative strengthening exercises have a significant correlation with longer postoperative walking distance and may improve early return to ambulatory function after THR (Gilbey et al. 2003; Wang et al. 2002; Whitney and Parkman 2002), others have shown that these exercises have no significant impact on the outcomes (Gocen et al. 2004; Rooks et al. 2006).
Surgical Approach
One of the factors influencing postoperative recovery and rehabilitation is the surgical approach. The patient’s gait may be compromised with approaches in which the hip abductors are altered (i.e., lateral or anterolateral approaches). Inadequate repair or weakness of the abductor muscles after these approaches may result in prolonged limping. The posterolateral approach spares the hip abductors but is associated with a slightly higher dislocation rate. This dislocation rate can be reduced with the use of larger femoral heads and proper repair of the posterior soft tissues (Pellicci et al. 1998; Woo and Morrey, 1982). The direct anterior approach, although theoretically appealing, is technically demanding and may require fracture table and intraoperative fluoroscopy (Peak et al. 2005). Minimally invasive THR has been widely marketed, but the claims of significantly reduced pain, less morbidity, better function, and improved patient satisfaction appear to be unfounded (Khan et al. 2009). Based on recent reports, minimally invasive THR does not appear to affect the short-term or intermediate-term outcomes after the THR (Howell et al. 2004; Inaba et al. 2005; Lawlor 2005). Complications of minimally invasive THR include wound-healing problems, component malposition, and increased risk of femoral fractures (Howell et al. 2004; Lawlor 2005).
Multimodal Pain Management
Severe pain after THR is one of the greatest fears patients have before surgery and is the leading cause of delayed discharge. Pain remains a poorly understood, complex phenomenon that plays a significant role in limiting patients’ functional recovery and participation in postoperative physical therapy (Ranawat and Ranawat 2007). Optimal pain control promotes earlier ambulation and faster return to normal gait (Singelyn et al. 1998). Decreased postoperative range of motion due to pain commonly contributes to arthrofibrosis and inferior results (Ryu et al. 1993). A multimodal pain regimen is a relatively new concept that has shown excellent results in terms of improving postoperative pain, reducing the need for narcotic medications and increasing patients’ motivation and participation in postoperative physical therapy (Brown et al. 2009; Busch et al. 2006; Hebl et al. 2005; Maheshwari et al. 2006; Peters et al. 2006). The key to multimodal pain control is the use of various pain medications with different mechanisms of action that results in superior pain control while minimizing their adverse side effects. Several postoperative pain control protocols exist, including patient-controlled anesthesia pumps (PCA), femoral nerve blocks (FNBs), continuous or one-time psoas compartment block (cPCB), and continuous lumbar plexus block (cLPB) (Becchi et al. 2008; Siddiqui et al. 2007). The use of local infiltration through an intra-articular catheter after THR has been shown to reduce the hospital stay and reduce the opioid-related side effects, such as nausea and vomiting, compared to continuous epidural infusion (Andersen et al. 2007). Local periarticular injections have also been used in a multimodal pain regimen that has been shown to reduce postoperative pain and improve patient satisfaction and functional recovery (Pagnano et al. 2006; Parvataneni et al. 2007).
Hip Precautions
Postoperative hip restrictions are used to protect the soft tissue repair after a posterior approach and thereby avoid hip dislocation (Masonis and Bourne 2002). Table 6-2 presents the common precautions associated with each surgical approach; however, variations may exist regionally. These precautions can be difficult to adhere to and may interfere with the postoperative rehabilitation process (Peak et al. 2005). Dislocation after THA through the posterior approach commonly occurs when the hip is adducted past midline, internally rotated, and flexed more than 90 degrees. To prevent this, an abduction pillow (Fig. 7-48 in Chapter 7) is placed between the patient’s knees while in bed or a small cushion can be situated between the thighs while sitting (Rao and Bronstein 1991). In some cases, especially in revisions or in patients who are noncompliant, it may be necessary to use knee immobilizers or hip abduction orthoses for 6 to 12 weeks postoperatively to restrict hip adduction and flexion (Venditolli et al. 2006).
Table 6-2 Precautions Associated with Total Hip Arthroplasty Surgical Approaches
| Surgical Approach | Precautions |
|---|---|
| Anterior | Do not extend hip beyond neutral. No lying in prone. Do not externally rotate and extend the hip. Do not perform the bridging exercise. |
| Posterior | Do not flex the hip greater than 90 degrees. Do not internally rotate the hip beyond neutral. Do not adduct the leg beyond neutral. |
After an anterior or anterolateral approach, extreme external rotation, adduction, and extension should be avoided. Several reports have shown that removal of hip precautions after the anterolateral approach results in a faster return to normal activities with higher patient satisfaction and no ill effects on short-term dislocation rates (Peak et al. 2005; Talbot et al. 2002).
Postoperative Total Hip Arthroplasty Rehabilitation Programs
Although a wide variety of exercise programs exist based on surgeon preference and geographic location, most protocols include quadriceps sets, gluteal sets, ankle pumps, and active hip flexion (heel slides) exercises (Enloe et al. 1996). Progressive hip abductor strengthening is also advocated, as the abductors maintain the pelvis level during the stance phase and prevent tilting of the contralateral hip during the swing phase (Enloe et al. 1996; Soderberg 1986). Most exercise programs address this issue initially by concentric hip abduction in a supine position and later through isometric hip abduction against resistance (Munin et al. 1995). The straight-leg raising exercise has been shown to apply a force of 1.5 to 1.8 times body weight and should be allowed only when partial or full weightbearing is permitted (Davy et al. 1988). If pain occurs, hip flexion and knee extension exercises can be done separately with placement of a bolster under the knee to minimize hip stress (Davy et al. 1988; Trudelle-Jackson et al. 2002). Several reports have shown persistent quadriceps atrophy or weak thigh flexors of the operated hip compared to the contralateral hip (Bertocci et al. 2004; Reardon et al. 2001; Shih et al. 1994).
Functional tasks of daily living targeted in the rehabilitation program include weight transfer to the nonoperated hip, gait training on both level and uneven surfaces, stair climbing, and lower extremity dressing. Transferring of weight to the uninvolved side is initiated by leading with the nonoperated limb both into and out of bed and then is progressed to both sides of the bed. This method is also used with stair climbing: Patients are instructed to lead with the uninvolved hip while ascending and lead with the operated hip while descending the stairs to optimize control of body weight through the uninvolved leg (Strickland et al. 1992).
Weightbearing
Weightbearing restrictions after hip replacement, such as toe-touch weightbearing (TTWB) or partial weightbearing (PWB), directly affect the level of functional independence after surgery. PWB refers to 30% to 50% of the body weight, but studies have shown that patients have difficulty estimating and maintaining this percentage and commonly violate the restricted weightbearing (Davy et al. 1988). In TTWB, no more than 10% of body weight should be applied. TTWB is preferred over nonweightbearing (NWB) because the latter may actually create greater pressures over the hip joint as a result of muscle forces maintaining the correct pelvic positioning (Davy et al. 1988). Full weightbearing (FWB) has been shown to promote faster recovery and shorter hospital stays (Kishida et al. 2001). This is a result of reduced reliance on the upper extremities for weightbearing, resulting in earlier strengthening of the operative hip abductors and improved functional outcomes.
Assistive devices such as walkers, crutches, and canes are used to unload the operated joint and provide support and balance (Holder et al. 1993; Strickland et al. 1992). Progression from one to another is dependent on several factors such as age, comorbidities, and weightbearing restrictions. Walkers are usually the first choice after THR and provide the greatest stability by increasing the patient’s base of support and unloading the affected leg (Davy et al. 1988). Because walkers require the use of both hands, carrying objects and performing self-care activities are challenging. In addition, walkers occasionally do not fit through doorways and are not recommended for use on stairs. Rolling walkers have higher self-selected walking speeds than standard walkers (Palmer and Toms 1992). Most patients advance easily from gait training with a walker to crutches or a cane. Axillary and forearm crutches are more appropriate for younger, more agile patients because they allow faster gait and yield better energy efficiency in NWB healthy subjects (Holder et al. 1993), but they have the least stability and require more control of the lower extremity and overall balance (Palmer et al. 1992). A potential complication of axillary crutches is axillary nerve compression injuries from incorrect use (O’Sullivan and Schmitz 1988). Canes are usually used on the contralateral side of the hip replacement and can transfer 10% to 20% of body weight by decreasing vertical hip contact forces (Brander et al. 1994; Deathe et al. 1993; Stineman et al. 1996). The basic function of a cane is to extend the base of support and to provide stability. Canes should be used only for patients who are fully weightbearing. Canes are inexpensive, allow a reciprocal walking pattern, can be used on stairs, and can be sized according to the patients’ height. The crook of the handle should be even with the radial styloid process when the elbow is flexed at 15 to 30 degrees (O’Sullivan and Schmitz 1988).
Levels of Rehabilitative Care
Different rehabilitation settings include acute hospital care, inpatient rehabilitation, skilled nursing facilities, and home or outpatient rehabilitation centers. Selecting the appropriate postoperative rehabilitation that best serves the patient is often confusing to both the patient and health care professionals. In acute hospital care, postoperative physical therapy is usually started on the same day of surgery or the next morning. The goals for the first physical therapy session are to assess the patient’s mobility status and to initiate therapeutic activities. With the patient lying supine in the bed, the physical therapist should observe the patient’s positioning, assess for signs of a deep vein thrombosis (DVT) (Table 6-3), note the state of the dressing, and record the ROM and strength of the uninvolved leg. If signs of a DVT are present or if there is excessive drainage noted on the dressing, the nursing staff should be immediately informed prior to continuing the treatment session.
Table 6-3 Signs Associated with a Deep Vein Thrombosis
| Lower leg swelling |
| Patient reporting pain in the calf and/or thigh |
| Redness in the calf |
| Pain reported by the patient when the calf and/or thigh are palpated |
Therapeutic exercises initiated during the initial visit may consist of lower extremity isometrics (quadriceps, hamstring, gluteal sets) and ankle pumps. Initially, a patient may be able to tolerate only passive ROM; however, he or she should be able to demonstrate increased active ROM tolerance over the course of the inpatient stay. Therapeutic exercises frequently are added daily to the patient’s routine. Table 6-4 presents a sample therapeutic exercise progression during the first postoperative week.
Table 6-4 Sample Week 1 Total Hip Replacement Postoperative Exercise Program*
| Postoperative Day | Prescribed Exercises |
|---|---|
| Day 1 | Isometrics (quadriceps sets, hamstring sets, gluteal sets) Ankle pumps |
| Day 2 | Continue previous exercises Supine hip range of motion within allowed ranges (passive to active as tolerated) Hip abduction active assisted to active range of motion Heel slides (heel toward buttocks) Bridging |
| Days 3–4 | Continue previous exercises Sitting heel raises Large arc quads |
| Days 5–7 | Continue previous exercises Mini-squats Standing hip flexion to 90 degrees (surgical leg) Standing hip extension (surgical leg) Standing hip abduction (surgical leg) Forward step-up |
* This sample program is based on a posterior surgical approach (see also page 435).
Comprehensive inpatient rehabilitation is different from acute hospital care because it is more focused on physical therapy and interdisciplinary treatment in combination with intensive family training. Inpatient rehabilitation is reserved for patients who require more than a few days of continuous skilled care, are able to physically tolerate at least 3 hours of therapy per day, and have a good chance of returning home within a reasonable time frame (Stineman et al. 1996). Medical management is similar to the acute hospital care setting. Reports have shown that older patients without family support and patients with comorbid medical conditions usually need inpatient rehabilitation after THR (Munin et al. 1995; Weingarten et al. 1994). The subacute nursing facility (SNF) was developed as a complement to inpatient rehabilitation and has grown as an alternative to it. The SNF is reserved for patients who cannot tolerate the 3 hours of therapy per day required in an inpatient rehabilitation program and are not at risk for medical instability (Haffey and Welsh 1995).
General criteria for home discharge include the following:
Postoperative protocol after primary total hip replacement
Management of Common Problems After Total Hip Replacement
Gait Faults
Gait faults should be watched for and corrected. Chandler (1982) pointed out that most gait faults either are caused by or contribute to flexion deformities at the hip. These faults generally are attributable to the patient’s attempts to avoid extension of the involved hip because such extension causes an uncomfortable stretching sensation in the groin.
Outpatient Total Hip Arthroplasty Physical Therapy Protocol
Exercises to increase muscle strength include the following:
Progressive overload to the muscles can be applied manually by the application of ankle weights or with the use of elastic resistance bands. The initial exercise prescription should consist of one to three sets of 15 to 20 repetitions. This volume of training will help to improve muscular endurance while minimizing the risk of excessive postexercise muscular soreness or pain. As endurance capacity increases, strength training can be increased to volumes of two to four sets of 6 to 10 repetitions. Table 6-5 presents frequently prescribed therapeutic exercises that address muscular weakness. The exercises are grouped by the muscles trained and in the order of difficulty.
Table 6-5 Therapeutic Exercises Frequently Prescribed in the Outpatient Orthopedic Physical Therapy Setting
| Muscle Group | Exercises* |
|---|---|
| Hip flexors | Isometric hip flexion Sitting hip flexion (no greater than 90 degrees initially) Manually resisted active hip flexion (patient supine, no greater than 90 degrees initially) Straight leg raise Standing hip flexion (no greater than 90 degrees initially) Standing hip flexion—full ROM when precautions are lifted. Multihip machine flexion |
| Hip extensors | Gluteal sets Bridging Manually resisted hip extension (patient supine with leg starting in a position of hip flexion) Standing hip extension Bridging with lower extremity extension Prone hip extension Multihip machine extension Forward step-up Mini-squats Lateral step-down |
| Hip abductors | Lateral heel slides (hip abduction supine) Manually resisted hip abduction (patient supine) Standing hip abduction Multihip machine abduction Side-lying hip abduction (when precautions are lifted) Lateral step-downs |
| Hip adductors | Hip adductor isometrics (with the patient supine and the hip in neutral or slightly abducted) Manually resisted hip adduction to neutral from a hip-abducted position Standing hip adduction (when precautions are lifted) Side-lying hip adduction (when precautions are lifted) |
| Hip external rotators | Manually applied hip external rotation isometric (patient supine in hook-lying) Manually applied hip external rotation with active hip external rotation from neutral (patient supine in hook-lying) |
| Hip internal rotators | Manually applied hip internal rotation isometric (patient supine in hook-lying with hip positioned in neutral or slightly externally rotated) Manually applied hip internal rotation with active hip internal rotation from a starting position of external rotation to neutral (patient positioned in supine) |
| Knee extensors | Quadriceps set Short arc quad Straight leg raise Large arc quad Forward step-up Mini-squat Lateral step-down Leg press |
| Knee curl | Hamstring sets Heel slides toward buttock Standing hamstring curls Leg curl machine (sitting): double-legged and single-legged curls |
| Gastrocnemius and soleus | Sitting heel raise Standing heel raise |
* Exercises are presented by their relative degree of difficulty.
Return to Sport After Total Hip Replacement
Physical activity levels may have an impact on the lifespan of the total hip replacement. Wear and tear on the replaced joint or a traumatic event may necessitate a revision surgery at a later date; however, having a hip replaced does not mean that one must end his or her recreational or sport pursuits. Exercise and activity are necessary for maintaining overall health. Instead of restricting activity, physicians have developed recommendations and guidelines for those who wish to return to activities that are more strenuous than walking. Table 6-6 presents examples of activities and sports, their associated levels of impact on the hip replacement, and recommendations as to the safety of performing and participating in a particular sport.
Table 6-6 Sport Participation Recommendations and Associated Levels of Impact on the Total Joint Replacement
| Level of Impact | Examples | Recommendations |
|---|---|---|
| Low | Stationary cycling Calisthenics Golf Stationary skiing Swimming Walking Ballroom dancing Water aerobics | Can improve general health Desirable for most patients, but may increase rate of wear Orthotics and activity modifications can reduce impact loads Concentration on conditioning and flexibility rather than strengthening |
| Potentially low | Bowling Fencing Rowing Isokinetic weight lifting Sailing Speed walking Cross-country skiing Table tennis Jazz dancing and ballet Bicycling | Desirable for most patients, but may increase rate of wear Requires preactivity evaluation, monitoring, and development of guidelines by surgeon Balance and proprioception must be intact Orthotics and activity modifications can reduce impact loads Emphasize high number of repetitions with minimal resistance |
| Intermediate | Free-weight lifting Hiking Horseback riding Ice skating Rock climbing Low-impact aerobics Tennis In-line skating Downhill skiing | Appropriate only for selected patients Require preactivity evaluation, monitoring, and development of guidelines for participation by surgeon Excellent physical condition is necessary Orthotics, impact absorbing shoes, and activity modification frequently necessary |
| High | Baseball/softball Basketball/volleyball Football Handball/racquetball Jogging/running Lacrosse SoccerWater skiing Karate | Should be avoided Significant probability of injury and need for revision |
From Clifford PE, Mallon WJ. Sports participation for patients with joint replacements based upon level of impact loading. Clin Sports Med 24(1):182, 2005. Table 1.
Table 6-7 provides a list of sports that are considered acceptable for participation, those that are possibly acceptable for participation, and those that are not recommended. Sports are designated “possibly acceptable” or “not recommended” based on the risk of falling or traumatic contact. Falling or experiencing traumatic forces may contribute to hip dislocation, hip fracture, or failure of the hip replacement.
Table 6-7 Sports Participation Recommendations for Patients with a Total Hip Replacement
| Acceptable | Possible | Not Recommended |
|---|---|---|
| Ballroom dancing | Ballet dancing | Baseball/softball |
| Bicycling | Calisthenics | Basketball |
| Bowling | Downhill skiing | Football |
| Cross-country skiing | Fencing | Handball/racquetball |
| Golf | Hiking | Karate |
| Horseback riding | Jazz dancing | Lacrosse |
| Ice skating | Jogging/running | Soccer |
| In-line skating | Rock climbing | Volleyball |
| Low-impact aerobics | Table tennis | |
| Rowing | Tennis | |
| Sailing | Water skiing | |
| Speed walking | ||
| Stationary cycling | ||
| Stationary skiing | ||
| Swimming | ||
| Walking | ||
| Water aerobics |
Adapted from Clifford PE, Mallon WJ. Sports participation for patients with joint replacements based upon level of impact loading. Clin Sports Med 24(1):183, 2005. Table 2.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


