Chapter 12 The Ankle and Foot
The ankle and foot perform two major roles: they support the body and propel it forward. In the process of performing these functions, several painful conditions may develop. Many of these develop in the forefoot and are often the result of poorly fitted shoes.
Anatomy
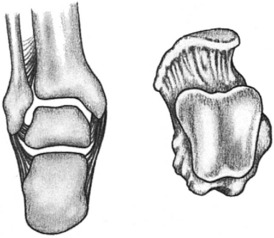
The ankle is a hinge joint composed of the articular surfaces of the lower portion of the tibia, talus, and medial and lateral malleoli (Fig. 12-1). The stability of this joint or “mortise” is maintained by the malleoli and their ligaments, which grasp the talus and prevent medial and lateral displacement. The talus and socket are both broader in front, an arrangement that provides maximum stability when the ankle is in dorsiflexion or neutral, and this prevents posterior displacement. Only movements of dorsiflexion and plantar flexion occur at the ankle.
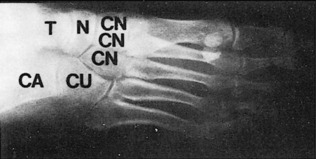
The foot is composed of 26 bones, 12 of which are components of the medial and lateral longitudinal arches (Fig. 12-2). Strong fascial supports maintain these arches and prevent collapse (Fig. 12-3). Eversion and inversion movements of the foot take place in the hindfoot at the subtalar joint. Injury or disease that affects this joint will cause pain in the region of the heel when walking on uneven or irregular surfaces. Abduction and adduction movements occur in the midfoot or midtarsal joints.

Flatfoot
ClINICAL FEATURES
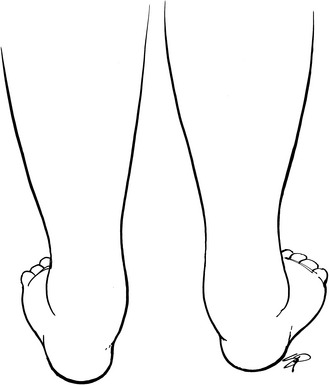
Symptoms are rare but may consist of pain, burning, and easy fatigability. With weight bearing, the heels are everted, and the forefoot appears pronated and abducted (Fig. 12-4). The child often “breaks down” the medial counter of the shoe. When it is not bearing weight, the foot often looks normal. Absence of the medial arch is apparent, and the foot is mobile without any fixed deformity. The child with flatfoot can usually form a good arch when asked to stand on tiptoe. The heel rolls into its usual varus position, and normal strength is apparent. A mild genu valgum (knock-knee) or internal tibial torsion may be present. With the heel inverted, passive dorsiflexion of the ankle will be limited if the heel cord is tight.

Fig. 12-4 Flatfoot deformity with eversion (valgus) of the heels and loss of the normal longitudinal arch.
A lateral roentgenogram taken with the foot bearing weight may reveal a loss of the normal arch and plantar flexion of the talus (Fig. 12-5). Some secondary bony changes may be present in the adult.

TREATMENT
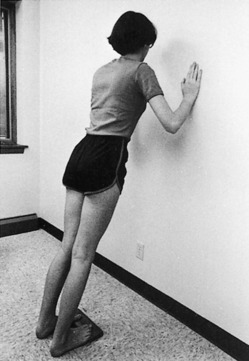
The treatment of flexible flatfoot in the child is controversial. The disorder is considered a normal variant in most cases, and only reassurance is needed. The natural history is spontaneous correction in the majority of cases with maturity. Symptoms are rare during childhood and uncommon even in the adult with moderately severe deformity. Actually, most foot pain in young adults is caused by an abnormally high rather than an abnormally low arch. Shoe corrections and orthotics used for this condition are of uncertain benefit. An arch cannot be “created” by supporting it. Exercises are of doubtful value, except for those that stretch the tight heel cords (Fig. 12-6). These exercises cure many cases associated with heel cord contractures. A soft arch support may be tried if symptoms are present. Surgery is reserved for symptomatic cases but is rarely necessary. No treatment is needed in most cases.
RIGID FLATFOOT
CLINICAL FEATURES
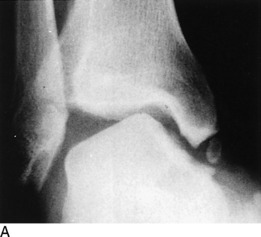
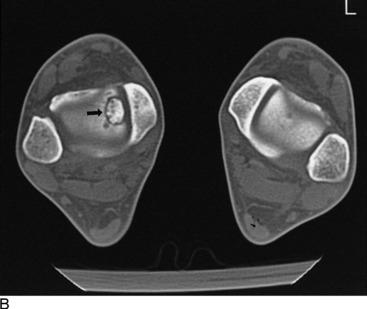
The onset of the disorder is usually gradual and begins in early adolescence if it is caused by a coalition. This may be because of the more solid ossification of the bar that occurs at this age. Stiffness and a painful limp are the most common initial symptoms. Tenderness and pain may be present over the peroneal tendons or in the hindfoot. The heel is frequently everted, and subtalar motion is limited and painful. The forefoot may be abducted. Passive stretching of the peroneal tendons by forefoot adduction and inversion frequently reproduces the pain. Swelling will be present if the disorder is secondary to a rheumatoid process. Roentgenograms may reveal arthritic changes in the hindfoot or the presence of a coalition (Fig. 12-7). Computed tomography (CT) and magnetic resonance imaging (MRI) are valuable in determining the extent of the condition.

POSTERIOR TIBIAL TENDINOPATHY/RUPTURE
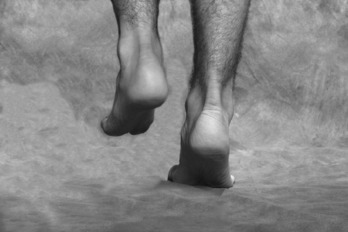
Further deterioration of the tendon could lead to rupture and the development of an acquired flatfoot deformity. Overuse, attrition, and failure are the cause. (Acute rupture of healthy tendon is unusual.) The condition is common, but the diagnosis can be difficult and is often missed until the patient discovers the loss of the arch. Usually, there is a history of previous pain, and the patient may have even had treatment for “tendinitis” in the same area. There is often only minimal pain after rupture, probably because the tendon is no longer attached and is no longer subject to stretch. Normally, the posterior tibial tendon locks the heel in varus, but without it, the heel does not move into inversion with push-off, and the gait is thus weakened. Clinically, the tendon sheath may be empty, and the heel everts with weight bearing. The medial arch is lower, and swelling and mild tenderness may be present. Inversion of the heel and forefoot against resistance is weak. There is also difficulty in performing the single heel rise test, in which the patient tries to rise on the ball of the foot on the affected side (Fig. 12-8). Heel valgus and forefoot abduction also increase gradually, and, as a result, when looking from behind, “too many toes” are visible with the patient standing (Fig. 12-9).
Clubfoot
CLINICAL FEATURES
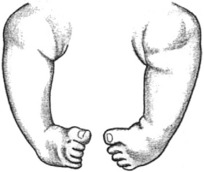
The deformity consists of three major components, none of which is passively correctable. This lack of correctability distinguishes clubfoot from other common foot deformities (which may be caused by intrauterine molding and usually resolve without treatment). The three components are equinus of the ankle and forefoot, varus of the heel, and adduction of the forefoot (Fig. 12-10). The medial border of the foot is concave, and the lateral border is convex.
Calcaneovalgus
CLINICAL FEATURES
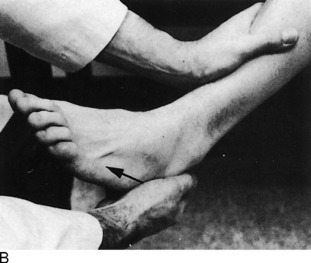
The deformity is easily diagnosed shortly after birth. Marked laxity of the ligaments of the foot and ankle is obvious, and the foot can often be dorsiflexed so that the toes touch the anterior aspect of the tibia (Fig. 12-11). The heel cord may appear to be severely stretched.

Kohler’s Disease (Osteonecrosis of the Tarsal Navicular)
The roentgenographic appearance is usually characteristic. Flattening, sclerosis, and irregularity of the navicular are usually present (Fig. 12-12).

Ankle Sprains
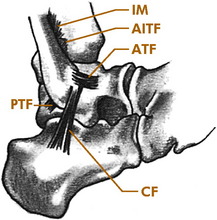
The sprain is the most common of all ankle injuries and may be the most common injury in sports. Most of these (85%) involve the lateral ligament complex as a result of excessive inversion. Medial sprains involving the deltoid ligament are rare. The anterior talofibular (ATF) ligament is usually injured first in the typical lateral sprain (Fig. 12-13). More severe injuries involve the calcaneofibular (CF) ligament. Only rarely is the posterior talofibular ligament involved. The injuries are often graded I, II, and III, with I being mild and II being moderate. Grade III injuries are more severe, with instability resulting from rupture of the ATF and CF ligaments. Inversion (varus) sprains may also cause marked hemorrhage of the peroneal muscles and even peroneal nerve damage. The subtalar joint may also be injured.
CLINICAL FEATURES
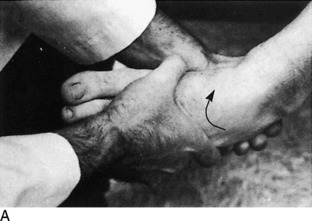
Physical examination is important. Hemorrhage and local tenderness are present at the site of injury. Careful palpation can localize the site of damage. Tendon function should be assessed, and any bony tenderness should be noted. The clinical evaluation of stability is sometimes helpful since it may determine the course of treatment, although this part of the examination may need to be deferred because of pain. Stability of lateral injuries can be assessed by the anterior drawer and talar tilt tests (Fig. 12-14). The anterior drawer is the most reliable test and least painful in the acute stage. Positive test results indicate complete rupture of the ATF and CF ligaments and a grade III injury. Motor function should always be evaluated.
Roentgenographic evaluation is always performed, and because the mechanism of injury that causes a lateral sprain is the same as that which causes an avulsion fracture of the base of the fifth toe, the film should include the fifth metatarsal base to rule out fracture of the small toe. If the injury is in a child or adolescent with open growth plates, tenderness over the fibular malleolus (even with normal roentgenographic findings) implies the more likely growth plate fracture rather than a lateral sprain, and a cast is usually necessary. Opinions vary on the usefulness of arthrograms, tenograms, and stress films (Fig. 12-15). A good clinical examination is usually sufficient to determine stability.

TREATMENT
Regardless of the severity, almost all sprains are treated nonoperatively. At first, all injuries are elevated, and a soft compression dressing is applied for comfort and to help control swelling. Ice (1 hour on, 1 hour off) is applied, and crutches are used for ambulation. Rest, ice, compression, and elevation (RICE) are continued for 1 to 2 days. Anti-inflammatory medication has been recommended in the past for these injuries because it was thought that suppressing the local inflammation could allow faster recovery from sprains and other similar soft tissue injuries. The use of these drugs under these circumstances has been the source of considerable debate, mainly because prostaglandins play important roles in the healing process and these medications block their production. The effects of NSAIDs on soft tissue healing are not clear, and any apparent benefits may only be because of their analgesic effects. Whether these drugs are helpful or harmful in these cases has not been determined. Crutches are frequently needed for 2 to 3 days. Heat is never used.
The next phase of treatment is rehabilitation, which includes early active range-of-motion exercises (circumduction) and weight bearing as tolerated (Fig. 12-16). “Alphabet” exercises (writing the alphabet in capital letters with the great toe) are begun, and in 4 to 5 days, exercise against resistance is added. Wrapping or bracing with a stabilizing orthosis may also be helpful. Static bicycling may be added after 1 week, along with fast walking.
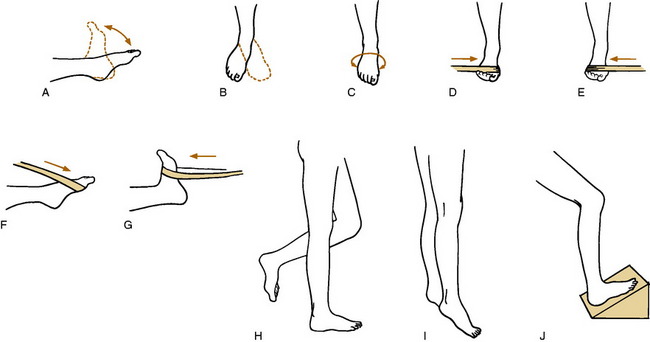
Fig. 12-16 Ankle exercises. A-C, Range of motion (dorsiflexion, plantar flexion, circumduction, and writing the alphabet with the great toe). D-G, Strengthening exercises using a rubber strap (invertors, evertors, plantar flexors, and dorsiflexors). H, Static one-leg standing with eyes closed. I, Toe raises. J, Heel cord stretches. Each exercise is performed 10 to 15 times. Ice is applied for a few minutes before and after each exercise period, and the exercises are performed 3 times each day.
NOTE: Lateral sprains of any severity may also cause lingering symptoms for weeks and months. Some syndesmotic sprains take even longer to heal (55 days vs 35 days for lateral sprains), and heterotopic ossification may even develop in the interosseous membrane. (Unless symptoms occur, long-term results are not usually affected by such ossification.) If healing seems delayed, the following conditions should be considered: (1) talar dome fracture, (2) reflex sympathetic dystrophy, (3) chronic tendinitis, (4) peroneal tendon subluxation, (5) another occult fracture—such as that involving the anterior superior process of the calcaneus or the lateral process of the talus, (6) poor rehabilitation, and (7) the high sprain. Evaluation at this point should start by another clinical examination and simply repeating the plain roentgenograms (Fig. 12-17). CT, bone scan, or MRI may be indicated at a later time.
Ankles that are chronically unstable because of lateral ligamentous laxity may benefit from the application of a 0.3-cm lateral heel and sole wedge to prevent inversion. Taping or bracing during vigorous activities is also helpful, as are strengthening exercises. Continuing symptoms may require surgical reconstruction of the lateral ligaments to relieve symptoms of instability, although late traumatic arthritis or chronic instability is rare regardless of treatment.
Tarsal Tunnel Syndrome
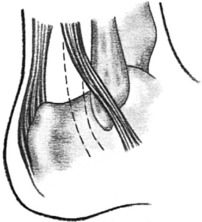
Nerve entrapment rarely may occur in the foot by compression of the posterior tibial nerve beneath the flexor retinaculum at the ankle. This retinaculum arises from the medial malleolus and inserts into the medial aspect of the calcaneus (Fig. 12-18). Space-occupying lesions, local tendinitis, traction injuries, fibrosis secondary to fractures, or deformities of the heel and foot can all compromise the tunnel and cause pressure on the posterior tibial nerve. The disorder is controversial, and there are many unanswered questions regarding its diagnosis and incidence.

Subluxation of Peroneal Tendons
Sudden, forceful dorsiflexion of the foot accompanied by contraction of the peroneal muscles may cause a tear in the retinaculum that holds these tendons in their groove behind the lateral malleolus. This may allow the tendons to acutely or chronically sublux over the lateral malleolus (Fig. 12-19). The condition can also follow a severe lateral ankle sprain.
Osteochondritis Dissecans of the Talus (Talar Dome Fracture)


Disorders of the Hindfoot
PLANTAR FASCIITIS (“PAINFUL HEEL SYNDROME”)
CLINICAL FEATURES
The pain is usually felt directly beneath the calcaneus but may be present in the area of the medial arch. The discomfort is characteristically worse with the first steps in the morning or after periods of prolonged sitting and later in the day after weight-bearing activities. Morning pain usually lessens as the foot “warms up.” Examination reveals local point tenderness in the area of involvement, usually the medial tubercle of the calcaneous. The pain may be aggravated by direct pressure or by maneuvers that place the fascia under a strain, such as dorsiflexing the toes and ankle. Some patients have a tight heel cord.
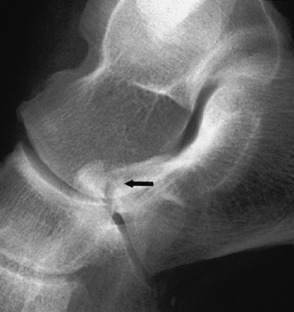
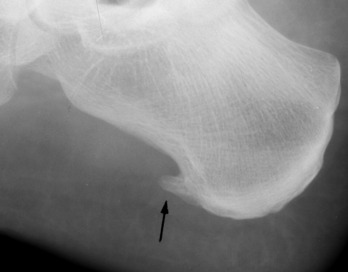
Roentgenographic findings are usually normal but may reveal a traction spur on the os calcis that is directed distally (Fig. 12-21). The significance of this osteophyte in the etiology of symptoms is unknown. It may be a response to muscle tension and is frequently found in the asymptomatic foot. It is not considered the cause of pain. A stress fracture or other bony disorder may need to be ruled out in some cases (Fig. 12-22).

TREATMENT
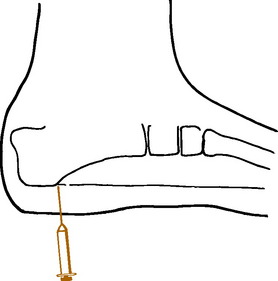
Taping, relief pads, heel cups, cushions, and various orthoses have all been used with only modest success. Over-the-counter pads and cups are as effective as more expensive orthoses. No treatment designed to cushion the heel seems to help, probably because heel strike may not be the cause of the problem. Exercises that stretch the heel cord and plantar fascia may help, but they should not be performed in the acutely painful foot. Only a gentle pulling sensation should be felt. Cold or ice as counterirritants may promote temporary relief. A heel lift or high-heeled shoe may relieve pain in some cases. Oral anti-inflammatory medication is used as necessary. Many patients will benefit from local infiltration of the tender area with a steroid/lidocaine mixture (Fig. 12-23). The injection may be repeated three to four times. (Avoid injecting the superficial tissue, which could cause fat pad necrosis.) Application of a short leg walking cast or removable cast-boot for 6 weeks is often very beneficial. Custom-fitted tension night splints that hold the foot in slight dorsiflexion are used in some resistant cases. Physical therapy is not usually recommended. Extracorporeal shock wave therapy has even been tried, but the results are inconclusive.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


