Chapter 12. The ankle and foot
SUMMARY
This chapter confines itself to common lesions in the ankle and foot arising from arthritis, trauma or overuse and begins with a presentation of the relevant anatomy and palpation techniques to aid their identification. Points from the history are considered and a logical sequence of objective examination is given, followed by discussion of lesions and suggestions for treatment and management.
ANATOMY
Inert structures
The inferior tibiofibular joint is the articulation between the fibular notch on the lateral aspect of the tibia and the distal end of the fibula. It is considered to be a syndesmosis because the firm union of the two bones is largely due to the interosseous membrane. Anterior and posterior ligaments reinforce the joint.
The deep part of the posterior ligament is the inferior transverse tibiofibular ligament which passes under the posterior ligament from the tibia into the malleolar fossa of the fibular. It is a thickened band of yellow elastic fibres forming part of the articulating surface of the ankle joint.
The firm union of the inferior tibiofibular joint is a major factor in the inherent stability of the ankle joint mortise. When the ankle joint is in dorsiflexion, the close packed position, the elastic nature of the inferior tibiofibular joint ligament allows the joint to yield and separate, accommodating the wider anterior aspect of the trochlear surface of the talus. In plantarflexion the ligament recoils as the narrower posterior aspect of the talus moves into the mortise, approximating the malleoli to maintain a pinch-like grip on the talus.
Dorsiflexion and plantarflexion of the ankle will induce small accessory movements in the inferior tibiofibular joint which in turn affect the superior tibiofibular joint. Injuries of the syndesmosis usually involve forced dorsiflexion, causing widening or diastasis of the ankle mortise (Edwards & DeLee 1984, Boytim et al 1991, Marder 1994). However, isolated injuries are uncommon and damage usually occurs in association with other major ligamentous disruption and fracture.
The ankle joint (talocrural joint) is a uniaxial, synovial hinge joint between the mortise, formed by the distal ends of the tibia and fibula, including both malleoli, and the dome of the talus. Its function is complex, with the talocrural, subtalar and inferior tibiofibular joints working in concert to allow coordinated movement of the rear foot (Hertel 2002). It bears more weight per unit area than any other joint, and any malalignment or instability may lead to degenerative changes (Sartoris 1994). The joint surfaces are covered with hyaline cartilage and surrounded by a fibrous capsule which attaches to the margins of the articulating surfaces. The capsule is lined with synovium and reinforced by strong collateral ligaments. The congruity of the articular surfaces during loading of the joint, the static ligamentous control and the dynamic control of the musculotendinous units all contribute to the stability of the ankle joint (Hertel 2002).
The collateral ligaments are roughly triangular in their attachments, radiating downwards from the malleoli to a wide base. Each has anterior and posterior components which link with the talus, and a central component that links with the calcaneus.
Movement at the ankle joint occurs about a transverse axis in a sagittal plane and amounts to approximately 20° of dorsiflexion and 35° of plantarflexion, allowing the foot to adjust to the surface on which it is placed. Dorsiflexion achieves the close packed position of the ankle joint and no movement of the talus in the mortise should be possible in this position. In full plantarflexion, the loose packed position, a small amount of side-to-side movement of the talus should be possible.
The medial collateral (deltoid) ligament forms a strong multiligamentous complex spreading out in a fan shape over the medial aspect of the ankle joint. It forms a continuous line of attachment from the navicular in front, along the sustentaculum tali to the talus behind. The origins and insertions of the various parts of the ligament are contiguous and therefore not clearly demarcated, but it is generally accepted to have deep and superficial fibres. The superficial fibres cross the ankle and subtalar joints, while the deep fibres cross the ankle joint (Boss & Hintermann 2002).
As the medial collateral ligament offers such strong support to the medial aspect of the ankle joint, traumatic injuries more commonly cause fracture and disruption of the syndesmosis rather than ligamentous injury. Most strain on the ligament occurs with a dorsiflexion and eversion stress. Biomechanical problems in the foot can, however, lead to a gradual onset overuse lesion of the medial collateral ligament and treatment should be directed to the cause.
The lateral collateral ligament consists of three separate bands which leave the ligament deficient in its support of the lateral aspect of the ankle joint. Consequently forced inversion of the plantarflexed foot commonly affects the lateral collateral ligament (Liu & Jason 1994, Lee & Maleski 2002).
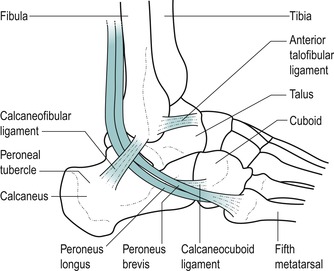
The components of the lateral collateral ligament are as follows (Fig. 12.1):
• The anterior talofibular ligament is an integral part of the capsule of the ankle joint. It arises from the anterior border and tip of the lateral malleolus and passes deeply and anteromedially across the ankle joint to the neck of the talus in the sinus tarsi. It is a wide, flattened band approximately the width of the patient’s index finger. In the anatomical position, the ligament runs almost parallel to the transverse axis of the foot, while in plantarflexion it runs more parallel to the vertical axis of the leg. In this position of plantarflexion, the ligament is most likely to be sprained particularly if the foot is inverted (Kannus & Renstrom 1991, Kumai et al 2002). It is the most vulnerable of the three components to a forced plantarflexion and inversion injury (Colville et al 1990, Hertel 2002)
• The calcaneofibular ligament is a narrow cord, separate from the capsule of the ankle joint. It arises from the apex of the lateral malleolus and passes obliquely inferoposteriorly, under the peroneal tendons, to attach to the calcaneus just behind the peroneal tubercle. Here it is closely related to the overlying peroneal sheath containing the tendons of peroneus longus and brevis (Marder 1994, Miller & Bosco 2002). This component of the ligament crosses both the ankle and subtalar joints and is vulnerable to varus stress; it is most taut in dorsiflexion and is most likely to be sprained with forced inversion in dorsiflexion (Colville et al 1990)
• The posterior talofibular ligament is a strong, thick band arising from the posterior border of the lateral malleolus and passing horizontally and posteromedially to the posterior aspect of the talus. Clinically, it is rare to find involvement of this ligamentous component.
 |
| Figure 12.1 Lateral collateral ligament of the ankle. |
The contribution of the individual lateral ligaments to ankle joint stability is not constant, but depends on the position of the ankle and foot in space. Ligamentous stabilization is most critical in the unloaded ankle as this is when injury tends to occur as initial contact is made with the ground during the gait cycle. During weight-bearing, stability is maintained by the bony congruency of the mortise. The anterior talofibular ligament has the weakest tensile strength with a load to failure two to three and a half times lower than that for the calcaneofibular ligament which is rarely injured in isolation (Boruta et al 1990, Miller & Bosco 2002).
The tibiofibular syndesmosis is established by the interosseous ligament, the posterior inferior tibiofibular ligament and the anterior inferior tibiofibular ligament, which is the weakest of the three. Post-traumatic antero-lateral laxity following injury to the anterior talofibular ligament may lead to anterior extrusion of the talar dome in dorsiflexion, resulting in impingement of the anterior inferior tibiofibular ligament (Bekerom & Raven 2007).
The foot consists of 26 bones and 57 joints which enable it to act as a rigid structure for weight-bearing, e.g. pointing in ballet, or to be converted into a flexible structure for mobility, e.g. gait activities (Nordin & Frankel 2001). The foot supports body weight and controls posture by maintaining the centre of gravity. It assists propulsion and lift, as well as restraining gait activities and acting as a shock absorber. To provide this variety of functions, arches have developed together with the joints, ligaments and muscles, all contributing to functional activities. The main joints and ligaments of the arches, of clinical concern in orthopaedic medicine, will be described briefly here.
The subtalar (talocalcaneal) joint is a synovial joint between the talus and underlying calcaneus, which works in conjunction with the ankle and mid-tarsal joints to form a functional component. These joints together allow the foot to adapt to the surface of stance and to act as a shock absorber. They allow adjustment of the arches of the foot and, in conjunction with muscle activity, provide spring and propulsion to gait. During walking, the subtalar joint adapts to the side-to-side slope of the ground, accompanied by secondary rotation of the tibia (Evans 1990).
The subtalar joint consists of separate anterior and posterior joint cavities divided by the sinus tarsi (a narrow tunnel running obliquely forwards and laterally between the talus and the calcaneus). Interosseous and cervical ligaments stabilize the subtalar joint and form a barrier between the two joint capsules; they have been described as the ‘cruciate ligaments of the subtalar joint’ (Hertel 2002). This division of the subtalar joint has implications for injection of the joint which will be discussed below.
Movements at the subtalar joint are complex due to the shape of the articulating facets, which allow a degree of play to occur simultaneously in three planes. The calcaneus ‘pitches’, ‘turns’ and ‘rolls’ (Kapandji 1987) under the talus, enabling these accessory movements to contribute to the functional movements of the joint. This results in triplanar motion of the talus around a single oblique axis. The subtalar joint, therefore, is a uniaxial joint with one degree of freedom of movement, supination, which achieves a varus position of the calcaneus, and pronation, which achieves a valgus position of the calcaneus (Levangie & Norkin 2001).
The mid-tarsal (transverse tarsal) joints consist of the calcaneocuboid joint laterally and the talocalcaneo-navicular joint medially. These joints adapt the posture of the foot, keeping the sole of the foot in contact with the ground whatever the slope of the surface or the position of the leg. Together they act as a shock absorber as well as providing elasticity and spring to gait.
The calcaneocuboid joint is supported by the dorsal calcaneocuboid ligament, which is a capsular ligament that runs along the dorsolateral aspect of the joint, and the plantar calcaneocuboid (short plantar) and the long plantar ligaments (Levangie & Norkin 2001, Palastanga et al 2006). The dorsal calcaneocuboid ligament is sometimes involved in an inversion sprain of the ankle as it resists inversion and adduction of the mid-tarsal joint.
The talocalcaneonavicular joint is supported by the spring ligament (otherwise known as the plantar calcaneo-navicular ligament) which spans the gap between the sustentaculum tali on the calcaneus and the navicular below the talar head. Consequently, this joint can be visualized as a ball and socket joint with the facet on the head and lower surface of the neck of the talus as the ball. The osseoligamentous socket is formed by the navicular anteriorly, the sustentaculum tali and calcaneus posteriorly and the spring ligament, and supports the head of the talus.
Movements at the mid-tarsal joint (calcaneocuboid and talocalcaneonavicular joint complex) do not occur in isolation (Levangie & Norkin 2001, Palastanga et al 2006). Accessory movements at the mid-tarsal joints consist of dorsiflexion and plantarflexion, abduction and adduction, and inversion and eversion.
A series of arches, ligaments and muscles satisfies the requirements of the foot to be able to provide both strength and mobility.
• The medial and lateral longitudinal arches are supported posteriorly by the calcaneus and anteriorly by the metatarsal heads. The talus forms the summit of the arch. The medial longitudinal arch is the larger of the two and has a dynamic role for gait. It consists of the calcaneus, talus, navicular, the cuneiforms and three medial metatarsals. It absorbs and transmits weight backwards through the calcaneus and forwards to the metatarsal heads, while providing elasticity for propulsion. The lateral longitudinal arch has a static role for weight-bearing. It is lower than the medial, making contact with the ground throughout its length to support load in standing. The main supporting mechanism for the longitudinal arches is the plantar fascia. Acting as a cable between the heel and the toes, it locks the joints of the foot and prevents the arches from collapsing during weight-bearing.
• The transverse arch is formed by the distal row of tarsal bones and the bases of the metatarsals, and acts to support and transmit body weight. As body weight is applied, the metatarsal bones separate and flatten slightly.
The arches of the foot depend on ligamentous and muscular support. The important ligaments are the long and short plantar ligaments, plantar aponeurosis and the spring ligament (plantar calcaneonavicular ligament). The intrinsic muscles of the foot maintain the arches, together with some of the long muscles of the leg. Tibialis anterior supports the medial arch, while peroneus longus supports the lateral arch.
The plantar fascia is a strong aponeurosis on the plantar surface of the foot which, together with the mid-tarsal ligaments and intrinsic and extrinsic muscles, withstands loading during weight-bearing. It consists of three variably developed components known as central, medial and lateral cords. The central cord is biomechanically the most important, arising from the medial side of the medial calcaneal tuberosity and consisting of longitudinally arranged fibres of collagen and elastin. The fibres pass distally into the forefoot, widening and thinning before dividing into five distinct bands that extend into the toes (Karr 1994, Yu 2000). At its insertion into the calcaneal tuberosity (the enthesis) it has a thickened ‘cuff’ similar in appearance to the rotator cuff of the shoulder (Yu 2000). This strong connecting cable passing between the pillars of the longitudinal arch has very little ability to lengthen, but under loading gives slightly to act as a shock absorber.
Contractile structures
The numerous tendons crossing the ankle joint complex contribute to dynamic stability as well as producing movement of the various joints. The lateral muscles have a role in controlling supination and the anterior muscles probably slow the plantarflexion component of supination, acting to prevent injury to the lateral ligaments (Hertel 2002). As tendons cross the ankle joint, they change their direction from running vertically to horizontally. Several retinacula prevent the tendons from bowstringing under activity, while synovial sheaths protect the tendons as they pass under the retinacula.
The talus provides attachment for ligaments and many tendons pass over it, although it does not itself give insertion to any contractile unit.
All anterior muscles of the lower leg are supplied by the deep peroneal nerve and their principal function is dorsiflexion of the ankle and extension of the toes.
Tibialis anterior (L4–L5) takes origin from the upper two-thirds of the lateral tibial shaft and adjacent interosseous membrane. It becomes tendinous in its lower third, passing across the anteromedial aspect of the ankle joint to insert into the medial aspect of the medial cuneiform and the base of the first metatarsal. Its function is to dorsiflex the ankle during the swing-through phase of gait and to invert the foot. It raises the medial longitudinal arch and works in conjunction with other muscles to counteract gravity and to control foot placement. This tendon runs a relatively straight course and is not a common cause of pain. However, hill running or irritation from tight-fitting boots, for example, may cause lesions of tibialis anterior (Frey & Shereff 1988, Chandnani & Bradley 1994).
Extensor hallucis longus (L5, S1) takes origin from the middle of the anteromedial border of the fibula and passes downwards and medially to a tendon which inserts into the base of the distal phalanx of the hallux. Functionally it dorsiflexes the ankle and extends the hallux to enable the big toe and foot to clear the ground during the swing-through phase.
Extensor digitorum longus (L5, S1) takes origin from the upper two-thirds of the anterior aspect of the fibula and passes downwards under the extensor retinacula, dividing into four tendons which insert into the dorsal digital expansions of the lateral four toes. Functionally, it assists dorsiflexion of the ankle and extends the lateral four toes, to clear the ground during the swing-through phase.
Peroneus tertius (L5, S1), a divorced part of extensor digitorum longus, arises from the lower anterolateral aspect of the fibula and inserts into the base of the fifth metatarsal. It functions as a weak dorsiflexor of the ankle and an evertor of the foot.
The peroneal muscles pass under two rectinacula to reach the lateral side of the foot. The principal function of the lateral muscles is to evert the foot, controlling side-to-side movements in standing and acting as the primary lateral dynamic stabilizers of the ankle (Frey & Shereff 1988). Peroneus longus, together with tibialis anterior, forms a stirrup for the foot, maintaining and supporting the arches. Both peroneus longus and brevis are supplied by the superficial peroneal nerve.
Peroneus longus is the main evertor of the foot and draws the medial side of the foot down, as in plantarflexion and eversion. Peroneus brevis also produces eversion and plantarflexion (Palastanga et al 2006).
Peroneus longus (L5, S1–S2), the more superficial of the two peroneal tendons, arises from the head and upper lateral two-thirds of the fibula. It becomes tendinous just above the ankle and passes behind the lateral malleolus in a sheath common to it and peroneus brevis. Continuing on, it crosses the lateral surface of the calcaneus, passing below the peroneal tubercle, where it leaves peroneus brevis. It occupies a groove on the lateral and plantar surfaces of the cuboid and crosses the sole of the foot obliquely to insert into the lateral side of the base of the first metatarsal and adjacent medial cuneiform.
Peroneus brevis (L5, S1–S2) arises from the lower lateral surface of the fibula. It lies in front of peroneus longus as the tendons pass behind the lateral malleolus in the common sheath. It crosses the calcaneus above the peroneal tubercle to insert into the base of the fifth metatarsal.
Generally, the more superficial posterior muscles are concerned mainly with plantarflexion of the ankle, while the deep muscles flex the toes. Both groups are supplied by the tibial nerve.
Gastrocnemius (S1–S2) is the most superficial of the posterior muscles and gives the calf its characteristic shape. It has two heads of origin from the appropriate posterior femoral condyle. The medial head is larger, extends more distally and is a common site for muscle belly injuries. The two muscle heads come together in a broad tendon which is joined on the anterolateral side by soleus, forming the Achilles tendon. Functionally, gastrocnemius flexes the knee and plantarflexes the ankle.
Soleus (S1–S2) lies deep to gastrocnemius, arising from the upper posterior aspect of the fibula and soleal line of the tibia. The muscle fibres blend into a membranous tendon which lies deep to the gastrocnemius, allowing both muscles to function individually. These tendon fibres then merge with the Achilles tendon.
Plantaris (S1–S2) arises from the posterior aspect of the lateral supracondylar ridge of the femur and descends medially to blend with the Achilles tendon. Its function is to assist gastrocnemius.
Gastrocnemius, soleus and plantaris form a functional group known as triceps surae; as well as functioning together they also have independent functions. Gastrocnemius works with plantaris to flex the knee and plantarflex the foot, providing propulsion to the push-off phase of gait. Soleus works continuously as a postural muscle through its slow-twitch muscle fibres which maintain the upright posture (McMinn et al 1995). In standing, the ankle is in a loose packed position with the centre of gravity falling anterior to the joint. Soleus counteracts the tendency for body weight to move forwards over the stationary foot (Standring 2009).
The Achilles tendon is a long tendon which receives the fibres of gastrocnemius and soleus. It is about 15 cm long (Standring 2009) and its insertion into the calcaneus is cushioned by two bursae: the retrocalcaneal bursa on its deep surface and the subcutaneous Achilles bursa on its superficial surface (Smart et al 1980). The tendon fibres twist as they pass down to their insertion into the middle of the posterior surface of the calcaneus. This twist in the tendon fibres is understood to be responsible for the tendon’s elastic properties, the stored energy providing propulsion to lift the heel during walking, running and jumping activities (Norris 2004). The tendon has a zone of relatively poor vascularity 2–6 cm above its insertion and is prone to overuse, degeneration and rupture, particularly at this site (Smart et al 1980, Chandnani & Bradley 1994).
Tibialis posterior (L4–L5) arises from the upper postero-lateral surface of the tibia. It passes behind the medial malleolus in its own sheath, crosses the deltoid ligament and inserts into the tuberosity of the navicular. It sends tendinous slips onto every tarsal bone except the talus. Functionally it is the main invertor of the foot, working with tibialis anterior. It gives support to the arches of the foot through its many tendinous insertions. It decelerates subtalar pronation after heel contact (Blake et al 1994). Activities which involve rapid changes in direction (e.g. soccer, tennis, hockey) place increased stress on tibialis posterior and make it vulnerable to injury in these situations (Frey & Shereff 1988).
Flexor digitorum longus (S2–S3) arises from the middle of the posterior surface of the tibia and passes downwards, becoming tendinous above the ankle joint. Behind the medial malleolus it is medial to tibialis posterior and occupies the groove under the sustentaculum tali. Dividing into four tendons, it inserts into the base of the distal phalanx of the lateral four toes. Functionally, flexor digitorum longus works with the lumbricals to keep the pads of the toes in contact with the ground, increasing the weight-bearing surface. It also acts to assist plantarflexion during the toe-off phase of gait, and repeated push-off activity may cause injury to this tendon (Frey & Shereff 1988).
The lumbricals (S2–S3) arise from flexor digitorum longus tendons and insert into the dorsal digital expansions. They flex the metatarsophalangeal joints and extend the interphalangeal joints; this counteracts the clawing tendency of the flexor digitorum longus. Together they maintain the medial arch.
Flexor hallucis longus (S2–S3) arises from the lower posterior surface of the fibula and passes behind the medial malleolus and under the sustentaculum tali to insert into the base of the distal phalanx of the big toe. It functions to provide the final thrust for toe-off and is important in supporting the medial longitudinal arch. Activities which involve repeatedly pushing off from the forefoot (e.g. ballet) may cause lesions in this tendon (Frey & Shereff 1988).
A GUIDE TO SURFACE MARKING AND PALPATION
Medial aspect (Fig. 12.2)
Palpate the short, thick, medial tibial malleolus, appreciating that the apex, anterior and posterior borders are all subcutaneous. Compare this with the longer, slender, lateral fibular malleolus which tends to project further distally and lie slightly more posteriorly.
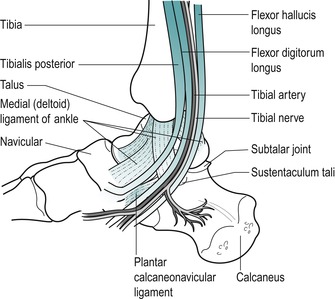 |
| Figure 12.2 Medial aspect of the ankle. |
It is difficult to palpate the tendons lying behind the medial malleolus, but from medial to lateral they are tibialis posterior, flexor digitorum longus and flexor hallucis longus ( Tom, Dick and Harry). You can palpate the posterior tibial pulse by applying light pressure behind the medial malleolus, approximately halfway between it and the Achilles tendon.
Consider the triangular medial (deltoid) collateral ligament which fans down from the medial malleolus to attach by a broad base from the navicular in front, to the talus behind.
Palpate the sustentaculum tali lying approximately one thumb’s width directly below the medial malleolus, where it feels like a horizontal, bony shelf.
Move directly forwards from the sustentaculum tali to the next palpable bony bump, the tuberosity of the navicular. This gives insertion to tibialis posterior and lies at the level of the lip of a slip-on shoe. Move directly forwards from the navicular to palpate the medial cuneiform and the base of the first metatarsal.
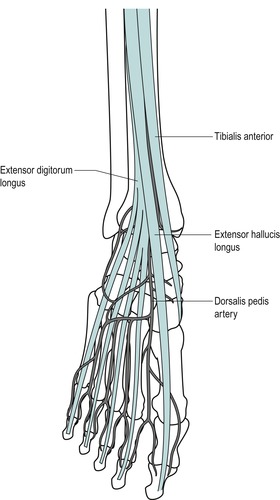
Anterior aspect (Fig. 12.3)
Place the ankle joint into plantarflexion and inversion, making the talus both visible and palpable anterior to the lateral malleolus. Palpate along from the anterior aspect of the lateral malleolus and the lower margin of the tibia to the anterior aspect of the medial malleolus to identify the ankle joint line.
 |
| Figure 12.3 Anterior aspect of the ankle. |
Move to the front of the lateral malleolus and feel the depression on the lateral side of the talus; this marks the entrance to the sinus tarsi (the narrow tunnel which runs between the talus and calcaneus in front of the subtalar joint).
Palpate the tibialis anterior, extensor hallucis longus, extensor digitorum longus and peroneus tertius tendons (from medial to lateral) as they cross the ankle joint anteriorly.
Palpate the dorsalis pedis pulse approximately halfway between the malleoli on the dorsum of the foot, just lateral to the tendon of extensor hallucis longus.
Posterior aspect (Fig. 12.4)
Palpate the calcaneus, the largest of the tarsal bones, which forms the bony prominence of the heel.
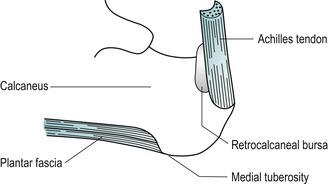 |
| Figure 12.4 Posterior structures of the ankle. |
Palpate the medial tuberosity of the calcaneus, which can be located at the posteromedial edge of the plantar surface of the calcaneus; deep palpation may be necessary. This marks the insertion of the middle cord of the plantar fascia (Fig. 12.5).
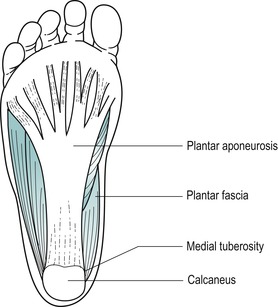 |
| Figure 12.5 Plantar fascia. |
Locate the insertion of the Achilles tendon into the middle third of the posterior surface of the calcaneus. Palpate the Achilles tendon, appreciating its thickness, and follow it up to the two fleshy bellies of the gastrocnemius; the medial belly should be felt to extend further distally than the lateral.
Lateral aspect (Fig. 12.6)
Palpate the lateral malleolus. Move approximately one finger’s width below it and slightly anteriorly to locate the peroneal tubercle. This tubercle varies in size and position so may not be obvious. It divides the tendons of peroneus longus and brevis.
 |
| Figure 12.6 Structures of the lateral aspect of the ankle. |
Consider the individual components of the lateral collateral ligament which take origin from the lateral malleolus. The anterior talofibular ligament is approximately the width of an index finger and it passes deeply, anteromedially to the talus. Its fibres run roughly parallel to the sole of the foot and it may be palpated in the region of the sinus tarsi. The calcaneofibular ligament passes obliquely downwards and backwards, under the peroneal tendons. The posterior talofibular ligament passes horizontally backwards to attach to the posterior talus; it is difficult to palpate.
Palpate the base of the fifth metatarsal and appreciate its prominent tubercle which gives attachment to peroneus brevis. Placing a thumb vertically behind the base of the fifth metatarsal will indicate the approximate position of the calcaneocuboid joint line. Placing another thumb or finger transversely across the tip of the thumb forms a T and the cross-bar of the T is resting over the dorsal aspect of the joint, indicating the approximate position of the dorsal calcaneocuboid ligament.
Position your hand to resist eversion of the foot, to aid identification of the two lateral tendons, peroneus longus and brevis. Behind the lateral malleolus, peroneus brevis lies in front of longus. They divide at the peroneal tubercle, with brevis running above the tubercle and longus below.
COMMENTARY ON THE EXAMINATION
Observation
Before proceeding with the history, a general observation of the patient’s face, posture and gait will alert the examiner to abnormalities, particularly of the gait pattern. A limp usually indicates abnormal weight-bearing, but a ‘short leg’ can produce a limp through functional discrepancies of hyperpronation and a flattened medial arch (Kannus 1992).
History (subjective examination)
The age, occupation, sports, hobbies and lifestyle of the patient may give an indication of the cause of the lesion and alert the examiner to possible biomechanical or postural problems.
The site and spread of pain help to localize the lesion, but, as a peripheral joint, pain is usually well localized. The presence of paraesthesia in the foot or pain in the calf or shin could suggest a more proximal lesion.
The onset of the symptoms may be sudden, due to trauma, or gradual, associated with overuse or arthritis. If the onset is traumatic in nature, the mechanism of injury should be established, particularly to give an indication of the ligaments involved. A ‘snap’ or ‘popping’ sensation at onset may indicate rupture of tendon, ligament or a fracture.
A minor injury is indicated by minimal pain and localized swelling, with the ability to continue weight-bearing activities. More severe injuries will produce diffuse swelling and an inability to weight-bear, suggesting ligamentous rupture or fracture.
The duration of symptoms indicates the stage of the lesion in the inflammatory process. A history of recurrent episodes indicates possible instability, requiring in-depth biomechanical assessment.
The symptoms and behaviour need to be considered. The behaviour of the pain indicates the nature of the lesion: mechanical lesions are eased by rest and aggravated by activity and weight-bearing.
Other symptoms described by the patient could include the ankle giving way; this is a symptom of ligamentous instability or possible loose body in the joint. A clicking or snapping sensation on the lateral aspect of the ankle could be due to disruption of the peroneal retinaculum, allowing subluxation of the tendons.
An indication of past medical history, other joint involvement and medications will aid diagnosis and establish whether contraindications to treatment techniques exist. Rheumatoid arthritis may affect the small joints of the foot. As well as past medical history, establish any ongoing conditions and treatment. Explore other previous or current musculoskeletal problems with previous episodes of the current complaint, any treatment given and the outcome of treatment.
Inspection
This should be conducted in both weight-bearing and non-weight-bearing postures.
Bony deformity and functional abnormalities, of the medial arch in particular, will usually manifest themselves in the weight-bearing position.
Check the height of the medial and longitudinal arches. Pes planus is a structural flat foot which is visible in both weight-bearing and non-weight-bearing positions, while a functional flat foot is only observed on weight-bearing.
The presence of functional flat foot can be generally estimated by looking for a difference in the height of the medial longitudinal arch in the non-weight-bearing and weight-bearing positions. Estimate the distance between the tuberosity of the navicular and the ground, first in a non-weight-bearing sitting position and secondly in the standing weight-bearing position (Evans 1990).
Observe the position of the Achilles tendon from behind for any deviations in the normal straight alignment, which would indicate postural deformity. Also notice if there is any angulation of the forefoot relative to the hindfoot.
Although it is important to note postural abnormalities of the foot, this should be kept relevant to the patient’s presenting signs and symptoms. A detailed biomechanical assessment is not necessary for uncomplicated lesions, but recurrent symptoms or failure to resolve the patient’s symptoms may require referral to a podiatrist or physio-therapy specialist in lower limb biomechanics.
A bony enlargement of the posterior superior calcaneus may be observed at the back of the heel, known as Haglund’s deformity, which may also be associated with bursitis and soft tissue swellings called ‘pump bumps’ (Stephens 1994) (see page 352).
It is worth inspecting the patient’s shoes for abnormal areas of weight-bearing. This is particularly relevant to athletes and should include their training shoes. In a normal gait pattern, wear is seen on the lateral side of the heel and the medial side of the forefoot (Kannus 1992). Camber running or worn-out or incorrect training shoes can alter angles of contact between the foot and the ground and be an external cause of overuse (Evans 1990). Advice will need to be given regarding the type of shoe best suited to the patient’s activities (Anthony 1987). Abnormal callus formation indicates abnormal weight-bearing.
Colour changes such as cyanosis, erythema or pallor may indicate circulatory involvement and a change in colour in transferring from the weight-bearing to the non-weight-bearing position should be further investigated by palpating for the presence of arterial pulses (Figure 12.7 and Figure 12.8). Bruising is often associated with a recently sprained ankle or gastrocnemius muscle belly lesion and tracks peripherally. A severe sprain of the ankle can cause traction injury of the superficial peroneal nerve and vascular structures. Consideration should be given to these possibilities if changes in skin colour persist (Acus & Flanagan 1991).
 |
| Figure 12.7 Palpation for dorsalis pedis pulse. |
 |
| Figure 12.8 Palpation for posterior tibial artery. |
Muscle wasting may be seen in the calf or peroneal muscles.
Swelling and any bruising on the lateral aspect of the ankle may be diffuse, indicating a moderate or major ligamentous lesion. Often a rounded mottled egg-shell-like swelling lies in front of the lateral malleolus: this is known as the signe de la coquille d’œuf (Litt 1992).
Minor swelling may be indicated by loss of the hollows behind the malleoli. Local swellings and ganglia should also be noted.
Palpation
As peripheral joints, the ankle and foot are palpated for signs of activity. The presence of heat is assessed (Fig. 12.9) and synovial thickening is palpated most easily along the anterior joint line (Fig. 12.10). Swelling is usually observed, but it is also possible to palpate for swelling, particularly around the malleoli. If the history indicates major ligament sprain, the malleoli and talus can be palpated for any focal areas of tenderness which may indicate a fracture (Lee & Maleski 2002).
 |
| Figure 12.9 Palpation for heat. |
 |
| Figure 12.10 Palpation for synovial thickening. |
State at rest
Before any movements are performed, the state at rest is established to provide a baseline for subsequent comparison.
Examination by selective tension (objective examination)
The suggested sequence for the objective examination will now be given, followed by a commentary including the reasoning in performing the movements and the significance of the possible findings. Comparison should always be made with the other side.
Ankle joint


Subtalar joint
• Passive varus of the calcaneus to produce supination (Fig. 12.13)
 |
| Figure 12.13 Hand position for varus and valgus stress, subtalar joint: valgus stress shown. |
• Passive valgus of the calcaneus to produce pronation (Fig. 12.13)
Mid-tarsal joints
• Passive dorsiflexion and plantarflexion (Figure 12.14 and Figure 12.15)
 |
| Figure 12.14 Passive mid-tarsal dorsiflexion. |
 |
| Figure 12.15 Passive mid-tarsal plantarflexion. |
• Passive abduction and adduction (Figure 12.16 and Figure 12.17)
 |
| Figure 12.16 Passive mid-tarsal abduction. |
 |
| Figure 12.17 Passive mid-tarsal adduction. |
• Passive eversion and inversion (Figure 12.18 and Figure 12.19)
 |
| Figure 12.18 Passive mid-tarsal eversion. |
 |
| Figure 12.19 Passive mid-tarsal inversion. |
Gross ligament tests
• Passive inversion in plantarflexion for lateral collateral ligament (Fig. 12.20)
 |
| Figure 12.20 Passive inversion in plantarflexion for lateral collateral ligament. |
• Passive eversion for medial (deltoid) ligament (Fig. 12.21)
 |
| Figure 12.21 Passive eversion for medial (deltoid) ligament. |
Contractile structures




Accessory ligament tests
• Drawer test for the anterior talofibular ligament (Fig. 12.26)
 |
| Figure 12.26 Drawer test for the anterior talofibular ligament. |
• Talar tilt test for the calcaneofibular ligament and integrity of the mortise (Fig. 12.27)
 |
| Figure 12.27 Talar tilt test for the calcaneofibular ligament and integrity of the mortise. |
• Test for the dorsal calcaneocuboid ligament (Fig. 12.28)
 |
| Figure 12.28 Test for the dorsal calcaneocuboid ligament. |
Toes
• Passive and resisted testing of the toes is not performed routinely, but is included if appropriate
Palpation
• Once a diagnosis has been made, the structure at fault is palpated for the exact site of the lesion
The objective examination is carried out in non-weight-bearing with the patient positioned comfortably in supine lying. The joints are examined first, assessing the range of movement, pain and end-feel. Passive dorsiflexion normally has a hard end-feel and to achieve end range it must be performed with the knee in flexion to take the tension off the gastrocnemius muscle complex, which spans both the knee and ankle joints. Passive plantarflexion normally has a firm elastic end-feel due to tension in the tissues on the dorsal aspect of the foot. The presence of the capsular pattern should be noted.
• Increasing limitation of supination.
• Eventual fixation of the joint in pronation.
• Limitation of adduction and inversion.
• Forefoot fixes in abduction and eversion.
• Gross limitation of extension.
• Some limitation of flexion.
• More limitation of flexion than extension.
• Joints fix in extension.
Although individual passive movements can be produced at the ankle joint, it is difficult to produce isolated passive movements at the subtalar and mid-tarsal joints. To assess the small range of movement available at the subtalar joint, grasp the calcaneus with both hands. Flex the knee to allow relaxation of the gastrocnemius complex and push the ankle joint into the close packed position. The varus and valgus stress is then applied to the calcaneus through the heels of both hands, using body weight. The amount of passive movement available at the subtalar joint is limited to a few degrees of supination and pronation and the normal end-feel is hard for both.
To assess movements occurring at the mid-tarsal joints, pull down on the calcaneus to place the ankle joint into dorsiflexion. Place fingers and thumb on either side of the first metatarsal, around the narrow, lateral aspect of the foot, and move the mid-tarsal joint through its range of passive movements, plantarflexion and dorsiflexion, abduction and adduction, inversion and eversion. These movements are minimal, and difficult to produce in isolation.
Assessing passive movements of the toes is not part of the routine ankle examination, but the movements can be applied as necessary to assess for the presence of the capsular pattern.
The most common injury to the ankle involves the lateral ligaments, but other injuries include lesions of the contractile units, subluxation of the peroneal tendons (through partial or complete rupture of the retinaculae), damage to the subtalar and mid-tarsal joints and injury to the various neurovascular structures crossing the region (Marder 1994, Lee & Maleski 2002). Anterolateral impingement is rare, occurring in only 3% of ankle sprains. It can arise from a meniscoid lesion, synovitis or impingement of the distal fascicle of the anterior inferior tibiofibular ligament (Bekerom & Raven 2007). Fractures and dislocations at the ankle are outside the scope of this book.
The main ligaments are tested by two gross composite movements: passive inversion in plantarflexion for the lateral collateral ligament and passive eversion in dorsiflexion for the medial collateral ligament. Should it be necessary, the ligaments can be assessed individually, and accessory tests can be applied for joint instability (see below and p. 334).
The contractile structures are assessed by resisted tests for pain and power. The joints are placed in the mid-position and maximum resistance applied. Resisted dorsiflexion tests mainly tibialis anterior and resisted plantarflexion tests gastrocnemius and the Achilles tendon. Testing the gastrocnemius group in lying may not produce symptoms and the test may need to be repeated in standing against the resistance of body weight. Resisted inversion tests mainly tibialis posterior and resisted eversion tests the peroneal muscles.
Accessory ligament and instability tests are applied if appropriate. The gross ligament test of passive inversion mainly tests the anterior talofibular ligament which crosses the ankle joint and is taut in plantarflexion. It is the most common ligamentous injury found at the ankle. It is further assessed by the drawer test which assesses its integrity (Marder 1994). Flex the leg to allow the foot to rest on the couch. Position yourself to view movement of the fibula on the lateral side of the ankle. Place one hand over the talus to fix it and the other just above the ankle joint. Apply pressure backwards against the fibula and tibia, comparing the degree of posterior movement of the fibula with the other side. Increased posterior movement of the fibula is a positive sign and indicates laxity or rupture of the anterior talofibular ligament. There is no standardized score for assessing abnormal displacement on the anterior drawer test, with some texts suggesting a grading system of 1–3 in excessive movement relative to the contralateral ankle. A ‘suction sign’ or dimple may be observed on the lateral aspect of the ankle if the anterior talofibular ligament is ruptured (Lee & Maleski 2002, Hattam & Smeatham 2010).
In a cadaver study, Beumer et al (2003) were unable to demonstrate significant displacement during various clinical tests, including the anterior drawer test, suggesting that syndesmotic injury is unlikely to be detected by such tests. However, the mean age of the 17 cadaver specimens was 78.4 years which may have had a bearing on ankle mobility and this was not addressed in the study. They conclude that pain rather than increased displacement should be considered as the outcome measure of these tests, but admit that how increased displacement relates to pain has not been demonstrated. Fujii et al (2000) similarly used elderly cadavers to assess the accuracy of the anterior drawer and talar tilt tests and, although both tests demonstrated reasonable displacement of the hindfoot, neither was sufficient accurately to diagnose specific ligament involvement. It was concluded that these conventional stress tests are not sensitive due to a substantial amount of difference between movement of the cadaver specimens, examiner agreement and positions of the ankle for the tests. To our knowledge, these ligament tests have not been evaluated in vivo.
The calcaneofibular ligament crosses both the ankle joint and the subtalar joint. Injury to this ligament does not often occur in isolation, but is usually in conjunction with the anterior talofibular ligament. The calcaneofibular ligament resists varus stresses to the calcaneus in dorsiflexion. Combined rupture of these ligaments results in an increased talar tilt (Boruta et al 1990, Wilkerson 1992, Marder 1994). With the knee straight, passively dorsiflex the ankle (this allows it to fall just short of the close packed position) and apply a strong varus stress to the calcaneus; compare the range of movement with the other side. This test may also be graded 1–3 relative to the contralateral ankle and again dimpling may be observed (Lee & Maleski 2002).
Disruption of the inferior tibiofibular joint may be due to a forced dorsiflexion injury which can cause widening (diastasis) of the ankle mortise (Marder 1994). In clinical practice, such an injury would usually only occur in conjunction with other major ligamentous damage and possible fracture, but the talar tilt test can also be applied to test the integrity of the mortise. Apply the talar tilt test as above (it can only be applied accurately if the lateral collateral ligaments are intact). If there is any widening of the mortise, pain and excessive movement will be appreciated. A ‘click’ may be felt as the talus tilts excessively in the enlarged mortise (Cyriax & Cyriax 1993, Hattam & Smeatham 2010).
The dorsal calcaneocuboid ligament crosses the calcaneocuboid joint, part of the mid-tarsal complex, and may be involved in a lateral collateral ligament sprain or injured in isolation. To assess its involvement, apply passive adduction and inversion of the mid-tarsal joints looking for increased pain.
CAPSULAR LESIONS
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


