The aging bony thorax
Steven Pheasant
Introduction
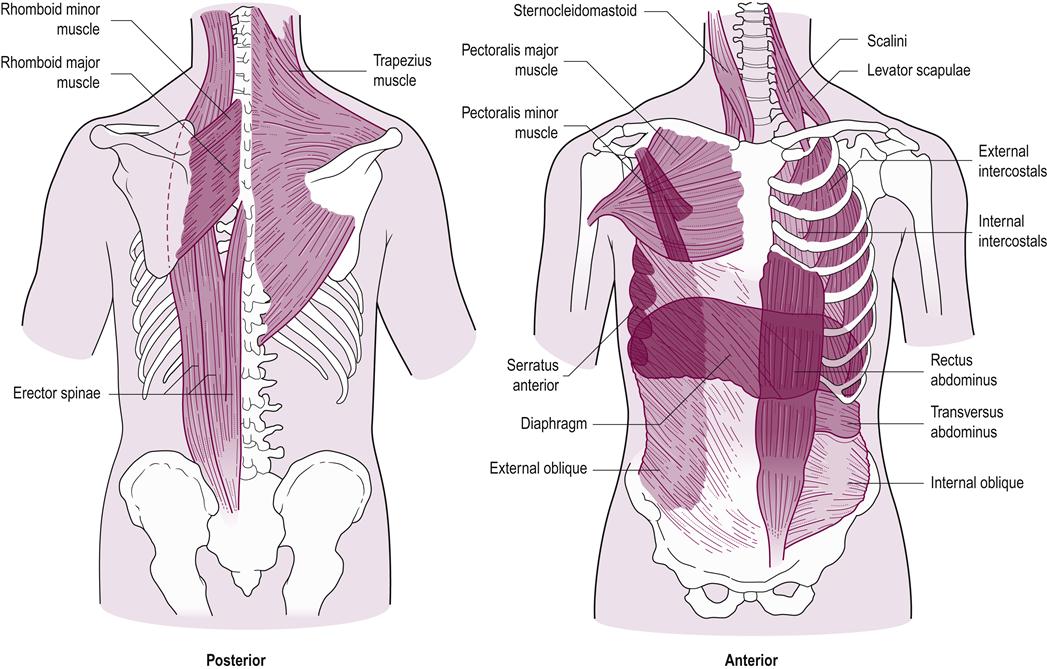
The bony thorax has the primary function of protecting the organs of circulation and respiration. Some protection is also given to the liver and stomach. Secondarily, the bony thorax contributes to the mechanics of breathing through the attachment of the muscles of respiration to the ribs. These elements are shown in Figure 23.1. Lastly, the bony thorax serves as the foundation from which the shoulder complex functions, therefore influencing the efficiency of the upper extremity (Edmondston et al., 2012).
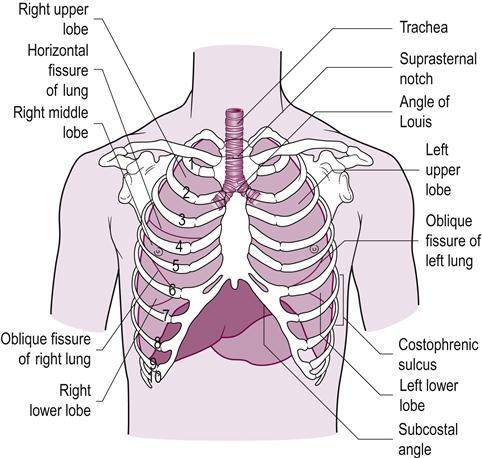
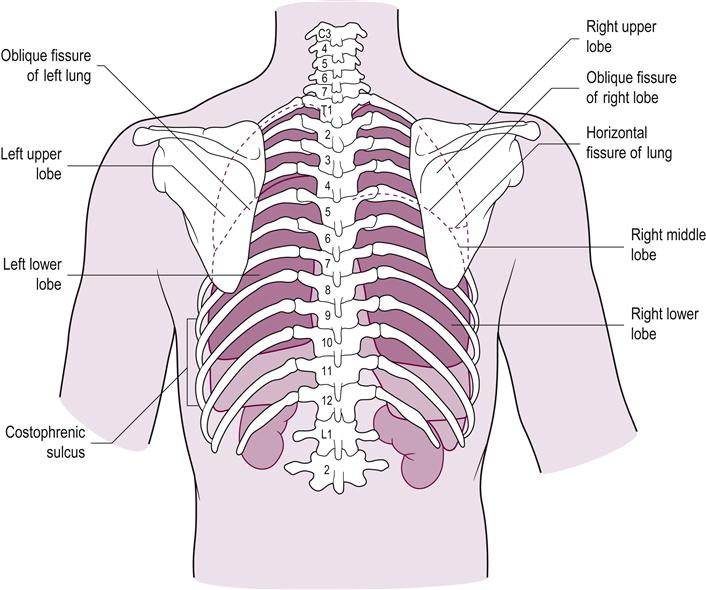
The thorax is composed of 12 thoracic vertebrae posteriorly, the sternum anteriorly and 12 pairs of ribs, which encircle the thorax. The first seven pairs of ribs are true ribs, with joints that attach the thoracic vertebrae to the sternum. The lower five pairs are considered false ribs since they do not attach directly to the sternum. Rib pairs 8, 9 and 10 attach to the sternum by way of their costal cartilage attachments to the seventh pair of ribs. Rib pairs 11 and 12 do not have attachments anteriorly to the sternum and are referred to as floating ribs. These bony relationships are shown in Figures 23.2 and 23.3.
The sternum is composed of three parts – the manubrium, the body and the xiphoid process – that are connected by fibrocartilage. The manubrium is the most superior and has notches for the clavicles. The body is a thin flexible bone and is the part used for closed cardiac compression. The xiphoid process is attached to the distal part of the body (Jenkins, 2009).
Each rib has a small head at the posterior end that presents upper and lower facets divided by a crest. Each facet articulates with the adjacent vertebral body. The next part of the rib, the tubercle, articulates with the transverse process of the corresponding vertebra. The shaft of the rib curves gently from the neck to a rather sharp bend called the angle of the rib. Successive ribs are separated by an intercostal space which is occupied by the intercostal muscles. The inferior border of each rib contains a costal groove in which the costal nerves and blood vessels run (Jenkins, 2009).
Kinesiology
Mechanics of the ribs
There are two basic kinds of rib movements. The pump-handle type is noted at the upper ribs, where movement is limited by joint articulations anteriorly and posteriorly. When the upper ribs move upward, because of the costosternal joints, the sternum follows by moving forward and gliding upward. This thoracic movement increases the anteroposterior diameter and depth of the thorax.
The lower ribs move outward and upward during inspiration. This movement increases the transverse diameter of the thoracic cage. The movement is similar to a bucket-handle movement and is given this name. These two movements (pump-handle and bucket-handle) increase the volume of the thorax, which contributes to the negative pressure responsible for air exchange during inhalation (Frownfelter & Dean, 2006; Jenkins, 2009).
The excursion of the ribs during both quiet and deep breathing has been observed to decrease with advancing age. The reduction in movement has been noted to particularly involve the excursion of the upper ribs during deep breathing, affecting the pump-handle mechanism, and a reduction in the lower rib during quiet breathing, affecting the bucket-handle mechanism. The reduction in rib excursion suggests a compromise of inspiratory capacity as a consequence of an aging thorax (Kaneko & Horie, 2012).
Muscles of the thorax
The primary muscle of respiration is the large dome-shaped diaphragm, which separates the thoracic and abdominal cavities. It has two halves, each of which has attachments anteriorly to the sternum at the posterior aspect of the xiphoid process.
Laterally, the diaphragm arises from the inner surfaces of the lower ribs and the lower six costal cartilages. Posteriorly, the diaphragm attaches to the vertebral bodies of the upper three lumbar vertebral bodies as well as the fascial coverings of the psoas major and quadratus lumborum. From these vast origins, the diaphragm spans the abdomen to insert into a central tendon at the pinnacle of the dome. The diaphragm descends as it contracts, increasing the vertical dimension of the thoracic cavity contributing to the negative pressure responsible for air exchange during inhalation (Frownfelter & Dean, 2006; Neumann, 2010).
The intercostal muscles also play a role in inhalation, are comprised of three layers of muscle and occupy the spaces between adjacent ribs. The most superficial layer is made up of the external intercostals, which have a fiber direction that traverses in an inferior and medial direction in a course similar to that of the external abdominal oblique muscle. The external intercostal muscles consist of 11 pairs corresponding with each intercostal space and attaching the inferior border of the superior rib to the superior border of the inferior rib. The intermediate layer is comprised of the internal intercostals, which have fiber orientations that resemble the internal abdominal oblique muscles traveling in an inferior and lateral fashion and also consists of 11 pairs. The deepest layer of the intercostal muscles is the intercostal intimi. Although less defined, their fiber direction is similar to that of the internal intercostals. These 11 external and 11 internal intercostals, along with the erector spinae, rectus abdominus, internal oblique abdominals and transverse abdominals, also contribute to respiration.
The external intercostals and portions of the internal intercostals have been reported to contribute to pump- and bucket-handle elevation of the ribs, therefore contributing to increasing both the anterior/posterior and lateral dimensions of the thorax during quiet inhalation, further reducing the negative intrathoracic pressure and aiding the flow of air into the lungs (Frownfelter & Dean, 2006; Neumann, 2010).
Postural stresses on the thoracic spine
The thoracic spine possesses a naturally occurring kyphosis. The kyphosis is, in part, due to the wedge shape of the thoracic vertebral bodies (taller dorsally and shorter ventrally). Both the magnitude of the thoracic kyphosis and the resultant postural stresses imposed on the vertebral bodies increase substantially with a forward-thrust head posture. Increased postural stresses render the thoracic vertebral bodies vulnerable to compression fractures, particularly in those who are osteoporotic. Compression fractures in the thoracic spine can lead to increased vertebral wedging, greater postural stresses and a progressive thoracic kyphosis that further compounds the impairment (Katzman et al., 2010). The incidence of thoracic compression fractures in those over 70 years of age is 19%, of which 30% will suffer multiple fractures due in large part to the above mentioned biomechanical factor (Waterloo et al., 2012). Information regarding vertebral compression fracture management and rehabilitation can be found in Chapters 24 and 25.
Pathologies involving the bony thorax
Obstructive Lung Diseases
Obstructive lung diseases cause an overinflated state in the lungs. The thoracic cage tends to assume the inspiratory position and the diaphragm becomes low and flat. The anteroposterior (AP) and transverse diameters of the chest are increased, and the ribs and sternum are always in a state of partial or complete expansion. In this population, the abdominal musculature assists expiration by forcing the diaphragm back to its resting position. This increased abdominal activity and the resultant trunk flexion movement may, in part, be responsible for the four-fold increase in vertebral compression fractures observed in those with chronic obstructive pulmonary disease (COPD) (Brunton et al., 2005; Frownfelter & Dean, 2006).
Restrictive lung diseases
In restrictive lung diseases, the lungs are prevented from fully expanding because of restrictions in the lung tissue, pleurae, muscles, ribs or sternum. The AP and transverse diameters of the chest should increase with inspiration, but do not increase to normal levels in these conditions. Interstitial fibrosis, sarcoidosis and pneumoconiosis are examples of disease processes that decrease elasticity (or compliance) of the lung tissue.
Tumors or abnormalities in the pleural tissue, such as pleurisy, pleuritis and pleural effusion, cause compression of the lungs. Any condition that elevates the diaphragm and prevents full excursion of this muscle diminishes the ability of the chest to expand. Examples of such conditions are ascities, obesity and abdominal tumors of any kind (Watchie, 2010).
Numerous musculoskeletal conditions cause disturbed respiratory mechanics. The autoimmune (collagen) diseases can affect any joint in the body, including the costochondral and costovertebral joints. Additionally, these are systemic diseases and thus can also involve the pleural or lung tissue as well. Rheumatoid arthritis, systemic lupus erythematosus and scleroderma are examples. Other less severe forms of autoimmune disease such as fibromyalgia and dermatomyositis may affect the musculature and can cause pain and restriction of the myofascial structures and thereby limit chest expansion.
Costochondritis is another common condition affecting the chest wall. The inflammation of the costochondral junction is often seen in individuals over 40 years of age and can be caused by coughing, strenuous exercise or physical activities that stress the upper extremities. Costochondritis is a self-limiting condition but can be a source of chest pain that may be mistaken for myocardial infarction. It can also be confused with the less common ‘Teitze syndrome’ that tends to be seen in a younger population (Proulx et al., 2009).
Orthopedic conditions such as kyphosis, scoliosis and kyphoscoliosis, affect primarily the vertebral segments and costovertebral articulations. Even with mild changes of spine alignment, the mechanics of the ribs and sternum are altered. In severe cases, the lung tissue, heart and major vessels may be compromised by the deformity and altered mechanics.
Scheuermann’s disease is characterized by hyperkyphosis of the thoracic spine and, though typically seen in adolescents, may not present until adulthood. Scheuermann’s disease is defined by three successive thoracic vertebrae demonstrating anterior wedging of>5° with management determined by the magnitude of the deformity. Long-term follow-up of individuals with thoracic deformity due to Scheuermann’s disease have a propensity for increased thoracic pain, decreased extension range of motion (ROM) of the thoracic spine and decreased strength of the thoracic spinal extensors. Individuals with a thoracic kyphosis exceeding 100° have also been shown to have reduced forced vital capacity due to compromised respiratory mechanics (Wood et al., 2012).
Ankylosing spondylitis can be considered in the autoimmune and orthopedic categories. It is considered separately here because of the severe consequences it can have on the thorax. In this condition, there is gradual fusion of spinal zygapophyseal joints, starting usually in the sacroiliac joints. As more and more of the spine becomes involved, X-rays demonstrate a bamboo-like image (bamboo spine). There is a calcification of the spinal segments as well as of the costovertebral joint, which causes severe restriction of chest expansion (Braveman, 2008).
Paget’s disease is a chronic condition that results in abnormal bone degradation and regrowth. The resultant bone has inferior structural properties and often results in bony deformity. Although the effects are not unique to the spine, the thoracic spine can certainly be involved, and the disease should be considered as a possible source of pathology in the aging spine (Lane, 2009).
Trauma, accidental or surgical, can cause muscle splinting which may restrict chest expansion or relaxation. After thoracic and cardiovascular surgery there is a tendency for the patient to breathe in a shallow, rapid and guarded manner, usually not using the diaphragm but, rather, accessory muscles such as the scalenes and sternocleidomastoids. Even after healing, the posture of such patients has often changed and shows an increase in thoracic kyphosis, a marked forward-thrust head, protraction of the shoulder girdles and an adducted and internally rotated position of the shoulders. The acquired posture compromises not only spinal and respiratory function but function of the upper extremities as well.
Another type of trauma to the thorax that is not often considered is injury that occurs in a motor vehicle accident. If the person is using a seat belt/shoulder strap type of restraint at the time of the accident, the shoulder strap may cause damage to the thoracic fascial structures, muscles, or sternum and ribs, as well as fractures. However, soft-tissue and joint injuries are often overlooked even though they may contribute to painful postural and respiratory dysfunction.
Compression fractures in the thoracic spine are commonplace in the geriatric population. The increased mechanical stresses that result from the forward-thrust head, rounded shoulder, kyphotic posture that frequently follows a thoracic compression fracture, predispose the individual to further pain, reduced spinal motion and compromised respiratory function (Waterloo et al., 2012) (see Chapters 24 and 25). A 9% reduction in forced vital capacity has been reported as a consequence of thoracic vertebral compression fractures. Additionally, multiple compression fractures may lead not only to increasing pain but to a protruding abdomen, thereby reducing abdominal cavity space. This could subsequently create difficulty with digestion. The deformity due to multiple compression fractures may also allow the floating ribs to rest upon the iliac crests, leading to another potential source of pain (Brunton et al., 2005).
When muscular, fascial, spinal, rib, or sternal components are the cause of restriction of lung capacity, the patient may benefit from physical therapy that can improve mechanics and lower the pain factor, thus improving quality of life in spite of the underlying disease process.
Assessment
History is very important. Understanding the underlying disease process or mechanism of trauma can help in defining the problem list and the goals for a particular patient. Histories of the present illness as well as of past medical and surgical problems are vital to proper examination and treatment. Laboratory and radiographic data, medication lists, particularly pulmonary and cardiac drugs, and psychosocial information should be gathered.
Examination can be broken down into components, starting with general appearance (Box 23.1). This consists of assessing level of consciousness, which can indicate adequacy of oxygenation of brain tissues. Body type is evaluated as normal, obese, or cachectic. An obese person has higher energy demands, even for simple activities. General appearance can also indicate whether the person is deconditioned. Also, some respiratory conditions are caused by excessive weight which can cause restriction of the diaphragm. The cachectic patient may have had weight loss associated with a carcinoma, or eating may take too much energy, so caloric intake becomes insufficient.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


