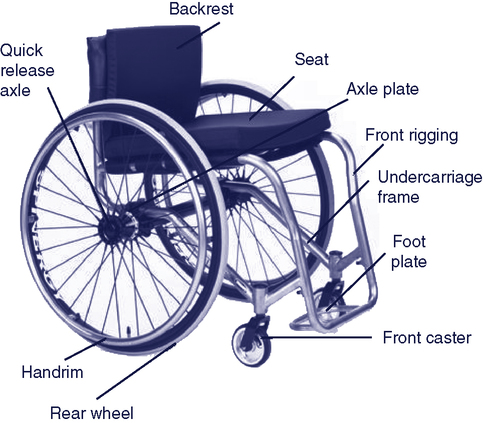
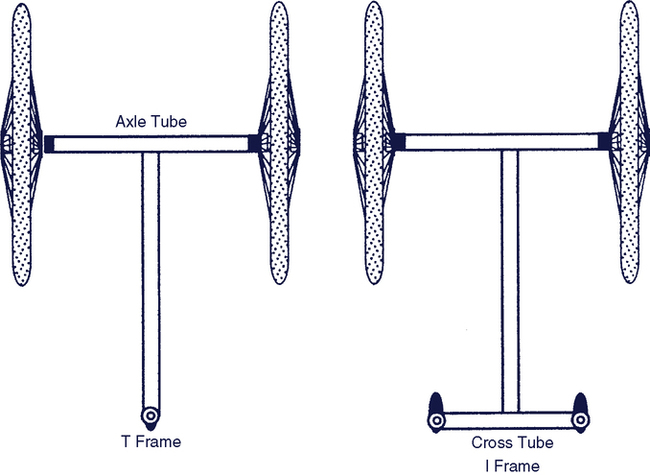
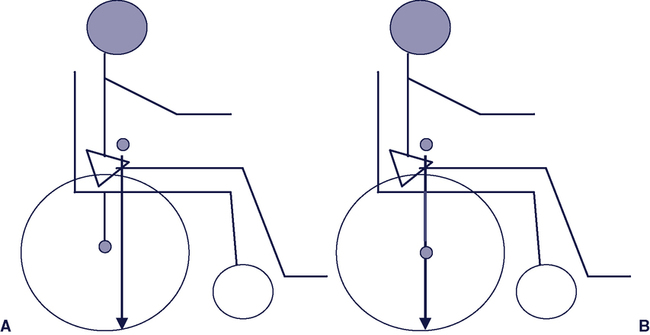
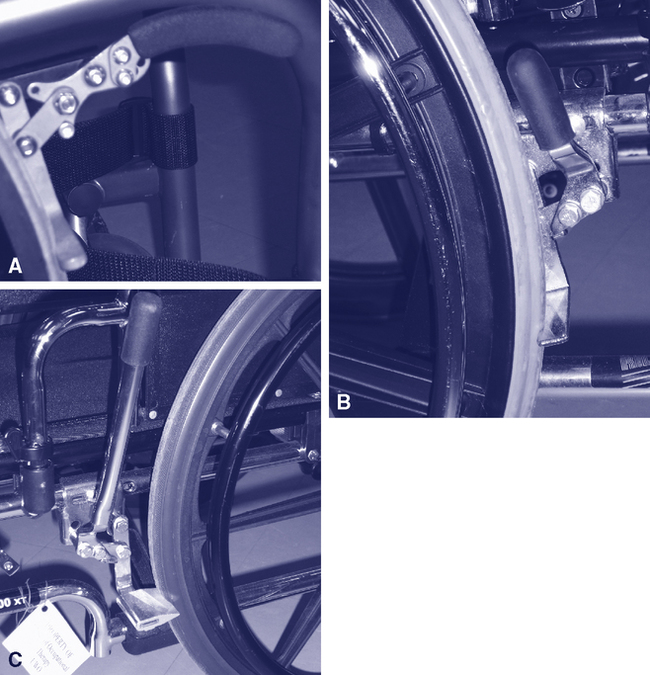
Upon completing this chapter, you will be able to do the following: 1. Discuss needs underlying evaluation of the consumer for a mobility system 2. Describe the three categories of mobility systems based on the need served by each 3. Describe the two primary structures of wheelchairs 4. Identify the major characteristics of manual wheelchairs 5. Identify the major types of powered mobility systems and their characteristics 6. Understand the influence of the relationship between the center of gravity of the user and the center of mass of the wheelchair on the function of the wheelchair 7. Describe the implementation phases for personal mobility systems There has been a significant increase in the number of individuals using mobility systems related to three different trends: (1) the increasing proportion of older adults in many countries, (2) rising rates of obesity, and (3) accessibility legislation. The population of most developing countries is aging, with the proportion of older individuals (65 years and older) expected to reach over 20% of the population in the United States by 20309 and earlier in Canada.5 Age-related physical changes, such as arthritis, result in mobility impairments that require the use of mobility devices. The proportion of morbidly obese individuals is rising, particularly in North America, which has resulted in the development of mobility devices that are specifically designed to support the increased size and weight of these individuals. Bariatric chairs are now available for those individuals whose mobility is impaired by obesity and related chronic diseases. Accessibility legislation in many countries has reduced the physical and institutional barriers to community participation of individuals with disabilities, with the result that more people are using mobility devices for instrumental activities of daily living. Data collected in the 2000 U.S. Census indicates that 20.9 million families in the United States have at least one individual with a disability living in their household.60 Of these, 16.6% report a physical disability that results in a functional limitation. A Profile of Disability in Canada, 2001 indicates that 13.7% of the Canadian population report a mobility impairment.15 Kaye, Kang, and LePlante (2002)30 provide information on the number of Americans who use mobility devices. These data are derived from the 1994–1995 National Health Interview Survey on Disability (NHIS-D). The survey indicated that 1.6 million Americans who live outside of an institutional setting use a mobility device. The vast majority of these individuals (1.5 million) use a manual wheelchair.30 Elderly individuals (65 years of age or older) have the highest rate of mobility use, accounting for 57.5% of manual wheelchair users and 69.7% of power wheelchair users.30 Kaye et al. (2002)30 present the top 10 conditions in the United States that result in use of a wheelchair or scooter. Individuals who have had a stroke are the leading group of mobility device users (11.1%).30 Additional neurological disorders that may result in mobility impairment include cerebral palsy, Guillain-Barré syndrome, Huntington’s chorea, traumatic brain injury, muscular dystrophy, Parkinson’s disease, poliomyelitis, spinal cord injury, spina bifida, and multiple sclerosis. Symptoms commonly seen in these neurological disorders are muscle weakness or paralysis, sensory deficits, and abnormal muscle tone. All these disorders can lead to limitations with joint range of motion, postural control, and mobility. The individual may also have cognitive and behavioral problems as a result of the disorder. Disorders that affect an individual’s cognitive functioning and ability to learn, such as Alzheimer’s disease and cognitive impairment, can also be associated with mobility impairments. In the first instance, dementia, the adult wheelchair user may require special consideration of safety measures if he has limited memory or insight concerning safe mobility. For example, as the cognitive impairment progresses, judgment can become impaired. A client at this stage may not recognize unsafe situations such as a stairwell and may attempt to propel the chair down the stairs, or the client may not be able to control anger and may use the wheelchair as a weapon and propel it into another person. In situations where cognitive impairment limits safe mobility, modifications are required to wheelchair skills training to simplify instructions and provide additional way finding cues in familiar environments. Measures such as use of seat belts may be used for safety, and consideration should be given to the ability of the caregiver to push the chair and lift and stow it when this assistance is required. A wheelchair seat belt may be considered a restraint in some jurisdictions. A summary of best practices for use of restraints is provided in Chapter 4. The World Health Organization’s International Classification of Functioning, Disability and Health (ICF)64 identifies mobility as an activity, rather than an impairment of a body structure or function. This system categorizes the source of the mobility impairment. For example, strength, range of motion (ROM), and endurance all have the potential to limit mobility. Another useful categorization scheme describes different abilities to ambulate.61 The degree of limitation in mobility varies across a broad scope, as shown in Box 12-1. At one end of the range are individuals who are considered marginal ambulators. At the opposite end of the range are those individuals who have severe mobility limitations and are dependent in manual mobility, with powered mobility being their only option for independence. Warren (1990)61 describes marginal ambulators as able to move independently in their environment but functional only at a slow rate or for short distances. Persons who have marginal ambulating skills can benefit from part-time use of a powered mobility device such as a scooter, which allows them to walk inside the home using a walker or cane and use a powered device outside the home to augment ambulation. Next are individuals who are exclusive users of manual wheelchairs. They may rely on a caregiver to propel the wheelchair or they propel a manual wheelchair using one of three methods: (1) using both upper extremities, (2) using both lower extremities, or (3) using an upper and lower extremity on the same side of the body (e.g., a person who has had a stroke). Marginal manual wheelchair users are able to propel a wheelchair manually but have upper body weakness, respiratory problems, or postural asymmetry as a result of pushing that limits their ability to propel a manual chair for a prolonged time.61 Marginal manual wheelchair users may also include individuals who formerly used a manual wheelchair for their mobility needs and have sustained an overuse injury from propelling the chair. Propelling a wheelchair for any length of time depletes the energy of these individuals and compromises their productivity in other areas of life. Marginal manual wheelchair users can benefit from powered mobility on a full-time or part-time basis. When an individual has a severe mobility limitation, powered mobility may be the best option to gain functional mobility. These individuals typically have a manual wheelchair, propelled by a caregiver, as a back-up chair. Powered mobility devices have the potential to enable the user’s participation in school, work, leisure, and other community-based activities. The control interfaces (see Chapter 6) that are available today make it possible for someone with only one or two movements (e.g., lateral flexion of the head or shoulder rotation) to operate a powered wheelchair; however, perceptual, cognitive, and behavioral impairments may prevent individuals from using a powered wheelchair even if they have the necessary motor skills. For example, a client with a visual-spatial impairment may have difficulty navigating a cluttered environment if she cannot maintain a safe distance from people or objects in the environment. When the individual also uses an augmentative communication system or an adapted van, integration of all of these devices is considered at the time of selection of the most appropriate mobility device. All mobility device users will require a system to support their seating needs (see Chapter 4). The use of powered mobility by young children is an area that has received a great deal of attention in the last decade. In the past, powered mobility was deemed inappropriate for young children for a number of reasons. These concerns were related to (1) the ability of children to operate a powered wheelchair safely, (2) the initial cost of the wheelchair and cost of replacing it as the child grows, and (3) possible detrimental effects on physical development if the child depends on a powered system instead of his own locomotion.32 Recent literature supports the provision of powered mobility to young children.25,50 Opportunities for early mobility have widespread benefits to the child, not only physically, but also cognitively and socially.17,50 Children who are able to move independently in their environment can initiate interactions with others; they don’t need to wait for another person to take them where they want to go. Most current literature suggests that affording the opportunity for mobility should occur at an appropriate developmental time. The goal of such mobility is not to learn how to control a chair, but to experience movement within the environment and to engage in relevant functional tasks, supported by mobility. As with any young child, it is the responsibility of the parent, caregiver, or rehabilitation assistant to ensure a safe environment in which the child can explore and experience mobility.50 Some needs that are specific to the older adult wheelchair user have been identified in the literature. Comfort, safety, increased function, and a feeling of security when moving in their environment have been identified as important needs related to seating and mobility for residents of long-term care facilities.40,43,44 The older adult wheelchair user may depend on another person to push the wheelchair. Therefore a mobility device that can be used easily by an attendant is important.27,58 Safety and security were deemed important for the user of the wheelchair, as well as for the care provider. For instance, it is important that the care provider be able to transfer a person in and out of the wheelchair safely. Both the user and the care provider will be more inclined to use a wheelchair that is comfortable, safe, secure, and easy to use. Wheelchairs that target the bariatric client are a recent development in wheelchair design. Bariatrics is a term that describes the practice of medicine concerning individuals who are significantly overweight. It is derived from the Greek baros, meaning weight, and iatrics, meaning medical treatment. In some situations, the client’s obesity is the cause of their mobility impairment. Obesity has become a major health problem in North America. The Center for Disease Control data10 report a growing trend in the prevalence of obesity (generally defined as a BMI of 30 or over). In 1995, the prevalence of obesity was less than 20% in all states. In 2000, 28% of states reported obesity prevalence of less than 20% and by 2005 this incidence had dropped to only 4 states. The 2005 figures further indicate that 17 states report a prevalence of obesity of equal to or greater than 25% and 3 states report a prevalence rate of equal to or greater than 30%.10 Diabetes is a serious chronic health condition that is associated with obesity. Mobility in this population is restricted by excessive weight, low physical endurance, cardio-respiratory complications, and complications arising from diabetes including vision impairment, circulatory and sensory impairments, and amputation. Typical wheelchairs have standard weight limits up to 300 pounds. Chairs for bariatric clients are capable of supporting weights up to 600 pounds and in some cases up to 1000 pounds. Examples of these chairs will be described later in this chapter. Clients who are morbidly obese present specific challenges when measuring for a wheelchair, as will be discussed later. The goal of wheeled mobility intervention is to support the user’s ability to move in his environments (i.e., the mobility output of the activity component of the HAAT model). Consistent with the HAAT model described in Chapter 2, the evaluation to determine the most appropriate wheeled mobility base starts with an assessment of the activities in which the individual wishes to engage while using mobility technology. Will the mobility device be used primarily to move from one place to another in the community, or will the individual use it as his primary means of mobility and consequently perform most activities (i.e., ADL and work and leisure occupations) while seated in the device? The rehabilitation assistant frequently interacts with an individual in the school, home, and long-term care (LTC) context. She has excellent opportunities in these settings to observe the activities in which the user wants and needs to engage. Further, the rehabilitation assistant is able to provide information on how an individual completes their activities, including the level of assistance required. For example, will the user complete these activities on his own, with the assistance of another person, and/or by using other technology such as an augmentative communication system? Box 12-2 identifies the factors that should be considered when selecting a mobility base for a consumer. Some of this information is available through the client’s chart or background information. The rehabilitation assistant provides information on the day-to-day function in other areas. For example, the daily interaction with the client by the OTA gives her a sound understanding of the client’s interaction with caregivers, behavior in different situations, impulsivity, skin integrity, and daily activities. The consumer profile provides background information about the client. Knowing whether an impairment is acute or long-term and relatively stable or progressive influences the choice of wheeled mobility. A client who has a progressive impairment such as amyotrophic lateral sclerosis (ALS) will lose function over time, so the rehabilitation assistant should be alert to signs that the wheelchair is no longer meeting the client’s needs. For example, a client whose motor function is declining may show fatigue when propelling a manual wheelchair over a distance that was easy for him to travel earlier. Alternately, a client who uses a joystick to control a power wheelchair may show loss of ability to reliably stop the chair or control its speed. Clients whose cognitive abilities are declining may become lost in familiar surroundings, use their chairs inappropriately to run into people or objects, or forget how to control the chair. Noting changes in a client’s weight or posture will also provide clues that the wheeled mobility device (and seating system) is no longer adequate. The individual’s physical and sensory skills are evaluated for range of motion, strength, motor control, skin integrity, vision, and perception. This assessment also includes determining the user’s optimal control site and interface for propelling the wheelchair. Information on the person’s weight and size is gathered in order to determine the size and capacity of the wheelchair. Measurements of the person’s leg length, thigh length, back height to base of scapula, back height to top of shoulder, and hip breadth are taken while the person is sitting. An obese person will need a bariatric wheelchair. Clients who are obese should be measured while sitting, as adipose tissue spreads when they lie down, resulting in an inaccurate measurement.16 If the consumer is a child and is expected to grow, that expected change needs to be reflected in the decision making as well. The person’s functional abilities are also evaluated. Two elements are important. The first is evaluation of different ADLs and Instrumental Activities of Daily Living (IADLs). IADL refers to those daily tasks that a person does to manager her life, for example banking, grocery shopping and use of transportation. In addition to identifying in which occupations the individual wishes to engage, this evaluation will determine how they complete those activities. The second element involves evaluation of wheelchair skills. The Wheelchair Skills Test (WST)* is a well-developed, standardized measure of various wheelchair skills.34,35 This test assesses the individual’s ability to perform basic wheelchair skills ranging from removal of an armrest and application of the brakes to more complex, advanced skills such as performing a wheelie in order to negotiate a curb. This test is one of the few that has had extensive research in all phases of its development. In addition to the evaluation, a training program has also been developed and evaluated. Information about this test and the training program are available at: www.wheelchairskillsprogram.ca. Institutional regulations and policies influence the recommendation of a mobility device. While the ATP is typically responsible for making a recommendation for a mobility device, the rehabilitation assistant is often responsible for the use of the mobility device in the institutional (e.g., rehabilitation facility or LTC) context. The rehabilitation assistant may be responsible for monitoring the client’s ability to use the chair safely, follow the policies and procedures of the institution regarding maintenance of the mobility device, and receive long-term training in device use (frequently with supervision of the ATP or other clinicians). Policies are established or being developed in some long-term care facilities that will limit the resident’s ability to use a wheelchair if they have repeatedly demonstrated use of the chair in a manner that threatens the safety of themselves or others in the environment.40 The rehabilitation assistant’s regular interaction with the client puts her in an excellent position to provide feedback on the client’s use of the chair and his potential to benefit from further training in wheelchair skills or from modification to the chair in order to promote its safe use. In this section we discuss the major characteristics of manual and powered mobility systems. Table 12-1 lists the major manufacturers of personal mobility systems. Modern mobility systems are more flexible and capable of being adapted to a variety of functional tasks. These adaptations may include height, tilt, recline, and axle-position adjustments, or combinations of any of these. The selection of a wheelchair is based on the evaluation discussed in the previous section and is a process of matching wheelchair characteristics to the consumer’s needs and skills.53 To meet the varied needs of individuals with mobility impairments, there are three broad categories of wheeled mobility systems: (1) dependent mobility, (2) independent manual mobility, and (3) independent powered mobility. Dependent mobility systems are propelled by an attendant and include strollers and transport chairs as well as a manual chair that is propelled by an attendant. A dependent mobility system is chosen when (1) the individual is not fully capable of independently propelling a wheelchair or (2) a secondary system is needed that is lightweight and easily transported. An independent manual mobility system is for those individuals who have the ability to propel a wheelchair manually. These bases have two large wheels in the back that allow the user to propel independently and two smaller front wheels. Independent powered mobility systems are required when the user has difficulty propelling a manual wheelchair. These are electrically powered wheelchairs that are driven by the user. There are many commercial options available within each of these categories to meet the needs of the individual user. In this section we discuss the characteristics of mobility systems, starting with the wheelchair’s two basic structures: a supporting structure and a propelling structure. Figure 12-1 shows the anatomy of a folding manual wheelchair. Figure 12-2 shows the anatomy of a rigid frame manual wheelchair. Table 12-1 Major Wheelchair Manufacturers The supporting structure of the wheelchair consists of the frame and attachments to it. Specialized seating and positioning (see Chapter 4) is often considered part of the supporting structure. Accessories to the frame (e.g., armrests, footrests) are also a part of the supporting structure. In some wheelchairs these accessories are manufactured as part of the frame. Some supporting structures are unique in that they are adjustable to allow for changes in the orientation of the user in space, including systems that provide tilt or support in a standing position. Frames may be either folding or rigid, and there are three common frame styles.11 Rigid frames are available in a box, cantilever, or T- or I-frame style. Typically the box frame construction (see Figure 12-3) has a rectangular shape that provides a strong and durable base to which the seat and wheels are attached. Lighter-weight designs are accomplished by replacing the box with a single bar extending between the wheels, forming a cantilever structure. Upright tubes from this main support are used to attach the seat and back. The footrests are extensions of the seat rails. As shown in Figure 12-3, the T construction uses a bar similar to the cantilever design but has a single bar attached to the center of the cantilever that connects to a single front caster. This configuration forms a T shape under the seat. If two front casters are used, then the T shape becomes an I shape. For transportation, the wheels on all these chairs are removed, and in some cases the back folds down. The choice between a rigid or box frame and folding frame styles involves a number of factors including the consumer’s needs, functional ability, method of transfer, and level of activity.11 The position of the axle of the drive wheel relative to the user’s center of gravity affects the stability and maneuverability of the wheelchair. Figure 12-4 displays this relationship. The center of mass of an empty wheelchair is located under the seat, in front of the drive wheels.21 When the user is seated in the wheelchair, the center of mass moves above the seat and forward or backward depending on the seated position of the individual relative to the drive wheels. When the center of mass is forward of the axis of the drive wheels, more weight is placed on the castors, making it more difficult to lift them.21 The chair is more stable but less maneuverable in this configuration. As the center of mass moves backward, closer to the axis of the drive wheel or even slightly behind it, stability decreases and maneuverability increases. Understanding this relationship is important when setting up the chair. An active user will want a configuration that is easily maneuverable and allows her to perform a “wheelie” (i.e., lift the castors up) to clear curbs and other barriers. A less-confident wheelchair user will be most comfortable with a chair that does not tip backward easily, allowing them to feel secure in their chair. Another fairly recent advancement in the wheelchair industry is the material used to form the chair frame. Much of the advancement in materials comes from the cycling industry. Wheelchair frames are made from many different materials including steel, aluminum, steel/aluminum alloys, titanium, and carbon fiber composites. These materials vary in their weight, strength, cost, how they conduct vibration, method of attaching components together, and how they are formed. Wheelchairs are classified according to a number of parameters including weight, adjustability, and available options. Standard wheelchairs are generally useful for very short-term use such as rentals at an airport or shopping mall.54 They are folding chairs, with very limited adjustment; in particular, the axle of the rear wheel is fixed. Features such as footrests and armrests may be fixed or detachable. There is limited choice of seat width and depth. They are the heaviest of the manual wheelchairs and therefore are not useful for long-term use as they require a great deal of energy to propel on a regular basis. Lightweight wheelchairs or lightweight high-strength wheelchairs54 weigh less than the standard chair, as their name would suggest. Otherwise, they tend to have similar features. These chairs offer more flexibility in choice of seat width and adjustment of back height. Both the standard and lightweight chairs are available with a lower seat to floor height that allows the user to propel with their feet. An ultra lightweight chair is substantially lighter than the standard chair. Schmeler and Buning54 suggest that the chairs in the standard and lightweight categories are not suitable for use over the long term. The ultra lightweight chair is one they consider useful for an individual who uses a manual wheelchair as her primary means of mobility. It retains the folding frame and is available with a lower seat to floor height for individuals who propel with their feet. The axle of the rear wheel is adjustable relative to the center of gravity of the user. Rigid sport ultralightweight wheelchairs54 are a huge growth area for the wheelchair industry. The primary difference between these and the previous categories is the rigid frame. These chairs have quick-release rear wheels and most have backs that fold down to facilitate transfer and storage of the chair in a vehicle. The axle of the rear wheel of these chairs can be adjusted relative to the center of gravity of the user. The implication of the position of the rear wheel axle relative to the user’s center of gravity for the stability and maneuverability of the chair will be discussed shortly. Leg rests and footplates support the legs and feet. Taken together, these two components are often called the front rigging of the wheelchair. Angle options are often available for the leg rests with either 90º or 70º hangers. These options increase the comfort of the user by accommodating his preferred knee flexion angle, but they can also add to the turning radius, which may be a factor for mobility in some environments. Leg rests may be fixed (built into the frame) or removable (swing away). Styles that swing away make it easier to transfer in and out of the wheelchair. Footplates are attached to the leg rests and are available as a single plate to support both feet or as two separate units, with individual height adjustment. The height of the footplate should support the desired position of the lower extremities. The angle of the footplate can also be adjusted to accommodate ankle flexion or extension. Heel loops can be attached to the back of the footplate to prevent the foot from sliding backward (see Figure 12-1). Wheel locks are the devices that prevent the wheels from moving during transfers and other stationary activities. They are available in a number of configurations, such as push or pull to lock, with lever extensions for individuals with limited reach; under-the-seat mounts; hill holders (devices that “hold” the wheelchair on an incline, preventing it from rolling downhill); and attendant controlled. Figure 12-5 (A–C) shows some of the various brake styles. The client’s preferred method of transfer and ability to access the wheel lock, the most reliable method available to manipulate the wheel lock, and the ability of the user or caregiver to maintain the wheel lock influence the selection of this component. As with the brakes of a motor vehicle, proper maintenance of the wheel locks is an important safety consideration. Wheel locks that are improperly maintained may not be in secure contact with the tire, causing instability, particularly during transfers or when holding the chair on an incline/decline. Anti-tip devices are small wheels, attached to a rod and mounted at the back of the chair. These devices prevent the chair from tipping backwards. When the drive wheels are located forward on the chair, anti-tip devices are recommended, particularly when the individual cannot safely perform a wheelie. Since these devices limit backward tipping of the chair, they can interfere with travel over some obstacles such as curbs. Anti-tip devices can be removed or rotated so they do not interfere with such travel when an attendant is pushing the chair. However, they should be returned to their original position when the user resumes propelling the chair.21 Anti-tipping devices can be seen on the back of the chair in Figure 12-9, which shows a composite mag wheel.
Technologies That Enable Mobility
Mobility needs served by wheelchairs
Disorders Resulting in Mobility Impairments
Functional Limitations of Mobility
Mobility Issues Across the Lifespan
Evaluation for wheeled mobility
Needs Assessment
Evaluation of the Human Factors
Environmental Factors
Physical Context
Institutional Context
Characteristics and current technologies of wheeled mobility systems
Manufacturer
Type of Wheelchairs
Web Address
Altimate Medical, Inc.
800-342-8968
Standing systems
www.easystand.com
Amigo Mobility International, Inc.
800-692-6446
Scooters
www.myamigo.com
Bruno Independent Living Aids
800-882-8183
Adult and pediatric scooters, sedan and van wheelchair lifts
www.bruno.com
Columbia Medical
800-454-6612
Dependent mobility bases
www.columbiamedical.com
Convaid, Inc.
Dependent mobility bases, transport chairs
www.convaid.com
ConvaQuip
Bariatric wheelchairs
www.convaquip.com
Etac (in the USA)
Balder USA, Inc.
888-422-5337
Independent manual wheelchairs for children and adults
www.etac.com
Freedom Designs
800-554-8044
Pediatric wheelchairs, tilt-in-space wheelchairs
www.freedomdesigns.com
Invacare800-333-6900
Manual, power, and sports wheelchairs
www.invacare.com
Levo USA, Inc.
888-538-6872
Manual and powered stand-up wheelchairs for adults and children
www.levo.com
Mulholland Positioning Systems, Inc.
800-543-4769
A variety of standing systems, pediatric wheeled bases and tilt bases
www.mulhollandinc.com
Otto Bock
800-328-4058
Pediatric seating and positioning, adult positioning, manual and power wheelchairs
www.ottobockus.com
PDG
888-858-4422
Wheelchairs for individuals with special needs, such as bariatric chairs, high agitation, and manual tilt wheelchairs
www.pdgmobility.com
Permobil, Inc.
800-736-0925
Stand-up powered wheelchairs; powered wheelchair with elevating seat; sports wheelchairs, lightweight manual wheelchairs
www.permobil.com
Pride Mobility Products Corp.
USA: 800-800-8586
Canada: 888-570-1113
Manual and electrically powered wheelchairs, scooters
www.pridemobility.com
Snug Seat
800-336-7684
Specialty bases for children and adults, car seats, dependent and independent mobility bases, pediatric wheelchairs
www.snugseat.com
Sunrise Medical
800-333-4000
Dependent and independent manual bases, sports wheelchairs, lightweight manual wheelchairs, powered wheelchairs, add-on power unit; adult and pediatric wheelchairs, tilt wheelchairs and scooters
www.sunrisemedical.com
TiLite
800-545-2266
Adult and pediatric titanium wheelchairs; manual wheelchair; sports wheelchair
www.tilite.com
Supporting Structure
Frame Types
Accessories
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Technologies That Enable Mobility