Teaching Visual: How to Interpret a Chest Radiograph
Irtza Sharif MD and Sean M. Studer MD, MSc
As with interpretation of other radiologic studies, reading chest radiographs should be approached by the novice reader in a systematic fashion. There are a few simple steps that the student may use to glean valuable information from a chest radiograph. This process begins with identifying technique, learning the features of the normal film (Fig. 18-1), and then methodically reviewing and characterizing the radiograph for apparent abnormalities.
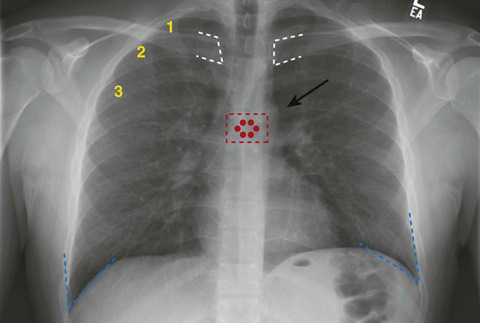
Figure 18-1 Normal chest radiograph (aka plain chest radiograph).
As with all films, one must first identify the type of film and the quality of the study; if these are appropriate, then one must systematically review the visible anatomic structures. For a chest radiograph, this includes the lung fields, the mediastinum, surrounding soft tissues, and the bony structures. There are also nonanatomic structures such as lines and implanted devices that should be reviewed. Keep in mind that the radiograph compresses three dimensions down to two, so there is loss of detail for which you need to account. Also, remember that the radiodensities of different structures in the chest may be the same, so the viewer often cannot differentiate between soft tissues. In fact, it is best to think of structures in terms of three densities: (1) air, (2) soft tissue and fluid, and (3) bone.
When interpreting the film, note the positioning of the patient and consider the direction of the radiation beam. Typically, radiographs are taken in one of three directions: AP, PA, and lateral.
 AP: the x-ray beam enters the front of the chest and hits the film, which is posterior to the patient (the portable chest radiograph is an AP study).
AP: the x-ray beam enters the front of the chest and hits the film, which is posterior to the patient (the portable chest radiograph is an AP study).
 PA: the x-ray beam enters the patient’s back and penetrates the chest before the film, which is placed along the patient’s anterior chest wall. The PA film is the preferred method of obtaining a chest radiograph, as it more accurately reflects the size of the cardiac and mediastinal silhouettes.
PA: the x-ray beam enters the patient’s back and penetrates the chest before the film, which is placed along the patient’s anterior chest wall. The PA film is the preferred method of obtaining a chest radiograph, as it more accurately reflects the size of the cardiac and mediastinal silhouettes. Lateral view (often combined with the PA view): the radiation beam usually enters the right side of the patient, with the patient’s left side against the film.
Lateral view (often combined with the PA view): the radiation beam usually enters the right side of the patient, with the patient’s left side against the film. Additional views (or variations in above styles) are also possible if you need to evaluate particular findings. An example is a decubitus view, which might be obtained so as to differentiate a pleural effusion from consolidation.
Additional views (or variations in above styles) are also possible if you need to evaluate particular findings. An example is a decubitus view, which might be obtained so as to differentiate a pleural effusion from consolidation.Regarding the quality of the film, it is important to consider penetration, rotation, and inspiration. Penetration refers to the adequacy of the radiation dose given to expose the film. This dose is variable, since patients’ body sizes (i.e., amounts of subcutaneous soft tissue) are variable. An inadequate radiation dose will make it difficult to evaluate denser tissues such as bone and soft tissue. A high dose may overexpose the less-dense lung tissue, making it difficult to differentiate subtle patterns. An easy way to determine if a film is properly penetrated is by looking at the mediastinum; the vertebrae and the spinous processes should be easily visible (note the red dots on Figure 18-1). Rotation of the film can be determined by looking at the distance of the medial head of the clavicles from the spinous processes; they should be equidistant if there is no rotation (note the white dashes on Figure 18-1). Examining adequacy of inspiration is a fundamental part of deciding if a chest radiograph is adequate. A good inspiration will allow you to see 6 or more anterior ribs, or 10 or more posterior ribs, above the right hemidiaphragm (note the yellow numbers on the right anterior ribs on Figure 18-1). We have started the count for you. How many anterior ribs do you count above the right hemidiaphragm?
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


