Teaching Visual: Coronary Angiography
Sidharth Yadav DO and Frank C. McGeehin III MD
Objectives
 Identify the major coronary arteries and their branch vessels.
Identify the major coronary arteries and their branch vessels.
 Identify right or left dominance.
Identify right or left dominance.
 Identify coronary anatomy on angiographic projections, and the related pathologies.
Identify coronary anatomy on angiographic projections, and the related pathologies.
Medical Knowledge
Coronary angiography remains the gold standard for visualization of the coronary anatomy when required in the clinical setting. The ultimate goal of coronary angiography is to define the coronary anatomy and to quantify or characterize the severity of coronary stenoses. Depending on the clinical scenario, recommending coronary angiography or, in general, cardiac catheterization requires appropriate patient selection and preparation.
Most indications for coronary angiography in the United States are for patients presenting with acute coronary syndrome or angina pectoris. Elective coronary angiography is usually performed after an initial cardiac workup of “chest pain” is abnormal, requiring more definitive diagnostic testing.
Coronary angiography is performed in a catheterization laboratory, which consists of a patient table, x-ray source, image intensifier, and a monitor display like that shown below (see Figs. 9-3 through 9-6). The x-ray source is below the patient. The image intensifier is the cylindrical structure directly opposite the x-ray source.
BASIC CORONARY ANATOMY
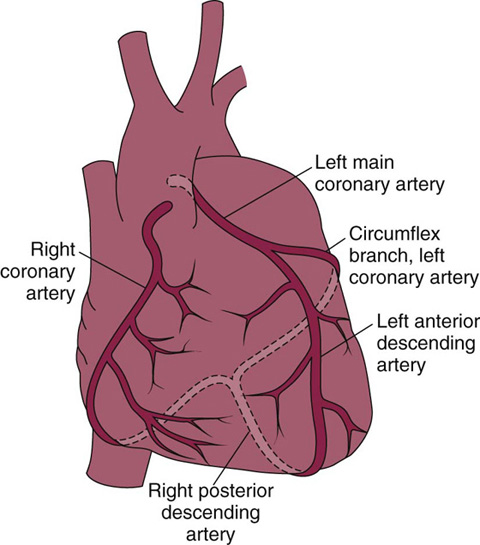
Interpreting coronary angiography requires basic understanding of coronary anatomy. The major epicardial vessels and their secondary branches are easily visualized on coronary angiography. The left main coronary artery arises from the left aortic sinus and usually bifurcates into the left anterior descending (LAD) artery and the left circumflex (LCX) artery. Generally, the LAD artery supplies the anterior/anterolateral walls and the interventricular septum of the left ventricle (LV). The LCX artery generally supplies the lateral/posterolateral walls of the LV. The right coronary artery (RCA) arises from the right aortic sinus and supplies the right ventricle (RV) and, in 85% of the population, gives rise to the posterior descending artery (PDA), which supplies the inferior portion of the interventricular septum. Anatomically, right or left “dominance” is determined by the artery that gives off the PDA. A small segment of the population is “left dominant,” indicating that the PDA originates from the LCX. Figure 9-1 is a basic schematic of the coronary anatomy.
“ANGIOGRAPHER’S” PERSPECTIVE
To effectively interpret coronary angiograms, one must understand that the heart is situated on an oblique axis in the chest cavity. Therefore, coronary arteries are best visualized from either a right or left oblique angle. The rotation, as well as cranial and caudal angulation of the image intensifier and x-ray source, allows us to perform comprehensive imaging while eliminating overlap and foreshortening of the arteries.
Oblique views can be thought of as turning the patient’s right or left shoulder toward the image intensifier. Nomenclature generally refers to the location of the image intensifier in relation to the patient’s long axis. Cranial and caudal angulations can be obtained by rotating the image intensifier along the long axis of the patient.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


