Surgical Decompression of Acute Compartment Syndrome of the Arm and Forearm
Bassem T. Elhassan
INTRODUCTION
Acute compartment syndrome may occur in any closed muscle compartment in the upper and lower extremity, and relates to elevation of the interstitial pressure in a closed fascial compartment with resultant microvascular compromise. The volar and dorsal compartments of the forearm are the most commonly affected in the upper extremity (1). The most commonly reported causes include supracondylar fracture in children and distal radius in adults (1,2). Outcome of surgical decompression of acute compartment syndrome is highly determined by early recognition and emergent surgical intervention (1,3).
INDICATIONS/CONTRAINDICATIONS
Indications
Surgical release of the arm and forearm compartments is indicated when the clinical diagnosis of compartment syndrome is made. Patients with compartment syndrome usually present with one or more of the following symptoms and signs: pain out of proportion to the injury with or without pain on passive stretch, sensory changes, weakness, vascular compromise, and paralysis (4). The diagnosis is confirmed when compartment pressures measure ≥30 mm Hg or compartment perfusion pressures (diastolic pressure minus compartment pressure) measure less than 30 mm Hg (5,6).
Contraindications
Compartment syndrome is an acute emergency, and for this reason, contraindications for performing surgical release are relatively uncommon. Bedside compartment release might be indicated in sick patients who are hemodynamically too unstable to be transferred to the operating room (4).
The main relative contraindication to perform surgical decompression is in patients whose blood coagulation profile is very abnormal that surgery may lead to uncontrolled bleeding.
The main relative contraindication to perform surgical decompression is in patients whose blood coagulation profile is very abnormal that surgery may lead to uncontrolled bleeding.
SURGICAL TECHNIQUE
Surgical approaches to release the affected compartments of the upper extremity require good knowledge of the anatomy of these compartments.
In the arm, there are two compartments: flexor (volar) and extensor (dorsal), which are encased by the brachial fascia and separated by the medial and lateral intermuscular septa (Fig. 14-1). The muscles of the volar arm compartment include the biceps, brachialis, and coracobrachialis. The dorsal compartment contains the triceps muscle.
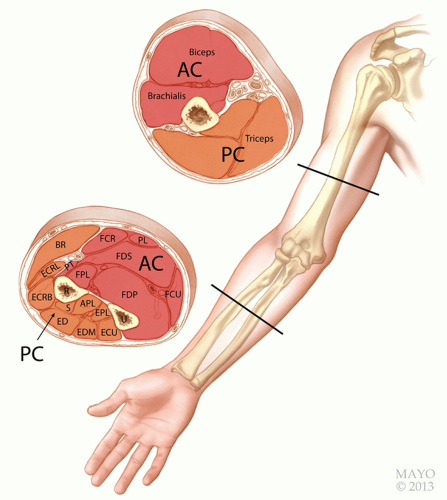 FIGURE 14-1 Cross section through the mid arm and forearm showing the two compartments in the arm and three compartments in the forearm with their included muscles. (AC, anterior compartment; PC, posterior compartment; R, radius; U, ulna; BR, brachioradialis; FCR, flexor carpi radialis; PL, palmaris longus; FDS, flexor digitorum superficialis; PT, pronator teres; FPL, flexor policis longus; FDP, flexor digitorum profundus; FCU, flexor carpi ulnaris; ECRL, extensor carpi radialis longus; ECRB, extensor carpi radialis brevis; Sup, supinator; ED, extensor digitorum; APL, abductor pollicis longus; EPL, extensor policis longus; EDM, extensor digitorum minimus; ECU, extensor carpi ulnaris.) |
In the forearm, there are three compartments: volar, dorsal, and lateral (mobile wad), which are encased by the antebrachial fascia (Fig. 14-1




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
