Weight bearer (n = 12)
Rower and axial rotator (n = 21)
Overhead thrower (n = 16)
Weight lifter (n = 24)
Miscellaneous (n = 7)
Olecranon (1)
First rib (2)
Clavicle (2)
Acromion (4)
Phalanx (1)
Scapula (1)
Ulnar shaft (3)
Lower ribs (16)
First rib (3)
First rib (7)
Ulnar shaft (3)
Distal radius (2)
Ulnar shaft (1)
Lower ribs (1)
Proximal humerus (1)
Distal humerus (2)
Scaphoid (3)
Radial shaft (1)
Distal humerus (5)
Ulnar shaft (2)
Metacarpal (1)
First rib (1)
Metacarpal (1)
Olecranon (4)
Sternum (1)
Scaphoid (4)
Distal humerus (1)
Sternum (2)
Proximal radius (1)
Coracoid (1)
A clear connection has been observed in rowers. All 11 rowers were diagnosed with stress fractures of the ribs. Ten of the 11 developed their stress fractures in the lower ribs. Five of 11 rowers developed stress fractures in multiple lower ribs. Like rowers, the axial rotator group showed a strong predilection for fractures of the ribs (7/10). Of the seven athletes with rib fractures, six occurred in the lower ribs with two athletes presenting with injury to multiple lower ribs. Among overhead throwers, patients showed a tendency for injuries around the elbow (9/16).
Weightlifters showed the greatest variability in anatomical location of injury, with injuries occurring as far proximal as the sternum and as far distal as the scaphoid. This group also showed a significantly disproportionate number of rib and shoulder girdle stress fractures (13/24). Notably, this group of patients sustained more injuries to the first rib (7/24) than any other group. A clear explanation for these injury patterns cannot be determined other than the variety of repetitive bending, torsional and axial loading forces applied to the thorax and upper extremity during weight training [10].
Stress Fracture of the Ribs
Rib stress fractures have been reported in several sports, including discus, rowing, rugby, golf, weightlifting, volleyball, gymnastics, judo, tennis, table tennis, baseball, basketball, soccer, javelin, backpacking, and wind surfing [4, 7]. Tensile muscular forces (rather than axial compressive forces) are predominantly responsible for rib stress fractures, as this is a non-weightbearing location [8]. The most common sites of fracture include the first rib anterolaterally, the fourth through ninth ribs posterolaterally, and the upper ribs posteromedially [10, 11].
First Rib
The sports most commonly associated with first rib stress fractures (Fig. 14.1a, b) such as baseball pitching, basketball, lacrosse, weightlifting, ballet, javelin, and tennis involve repetitive overhead positioning of the arm [7, 12, 13]. Patients with first rib stress fractures present with insidious onset of dull, vague pain in the anterior cervical triangle and mid-clavicular region, with occasional radiation to the sternum and pectoral region [11]. Repetitive scalene muscle contractions elevate the first rib, while serratus anterior and intercostal muscles depress it [14]. These opposing forces generate bending and torsional forces leading to microtrauma. Prisk and Hamilton [15] proposed the “trapezius squeeze test.” This test involves applying pressure to the anterior trapezius muscle, causing involuntary contraction of the muscle and eliciting rib pain. This test was found to be reliable for diagnosing first rib stress fractures on physical examination in five cases of stress fractures in ballet dancers [10, 15].
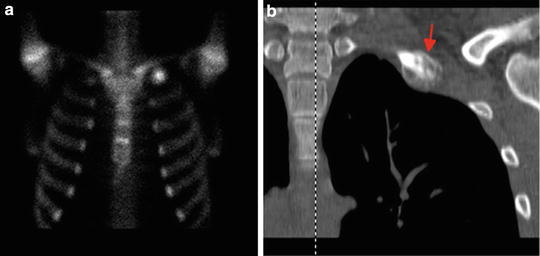
Fig. 14.1
Bone scan (a) and coronal CT scan (b) images demonstrating left first rib stress fracture in a male collegiate gymnast. CT scan demonstrates healing with abundant callus formation
Second Through 12th Ribs
Repetitive strain on the torso is a cause of middle- and lower rib stress fractures (Fig. 14.2a, b), and these are most commonly described in athletes involved in rowing, discus, and golf [6, 7, 14, 16, 17]. Patients present with increasing lateral chest pain and are diagnosed most commonly by radionuclide scans [16]. Other athletic activities associated with these fractures include tennis, gymnastics, and throwing sports [4, 7]. Among rowers, fractures are found most commonly between the fifth and ninth ribs, and pain generally is greatest at the finish of a stroke and may be exacerbated by coughing, sneezing, or deep inhalation [7, 10, 14]. Among golfers, Lord et al. [18] described 19 cases of rib stress fractures. Sixteen of the 19 golfers sustained injury on the leading arm side of the trunk. The posterolateral aspects of the fourth through sixth ribs were the most commonly injured sites [18]. The authors suggested that the ribs on the leading arm side are most commonly involved because of repetitive contraction of the serratus muscle through all phases of the golf swing on the leading side compared with the trailing side [18].
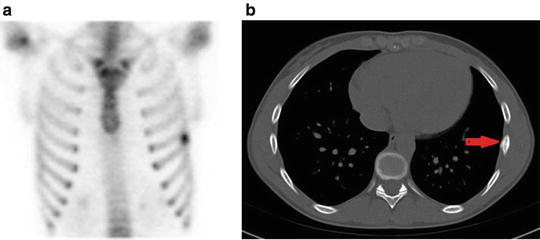
Fig. 14.2
Bone scan (a) and axial CT scan (b) images demonstrating stress fracture of the left mid seventh rib. CT scan demonstrates fracture callus present
The treatment of rib stress fractures is nearly always nonoperative, with the initial goal being to provide symptomatic relief. In general, rib stress fractures rarely fail to heal with modification or complete discontinuation of the causative activity for 4–6 weeks [4]. Treatment includes relative rest by avoiding overhead lifting, throwing, or rowing sports. Nonunion of the ribs (Fig. 14.3) has been described, but this is very rare and may be asymptomatic [4, 15].

Fig. 14.3
Anteroposterior chest radiographs demonstrating nonunion (Grade 5) of the right tenth rib stress fracture in a male collegiate rower
Sternum
Figure 14.4 shows the coronal and sagittal MRI images of a 28-year-old male competitive weight lifter with a midsternal stress fracture. Stress fractures of the sternum may be diagnosed on radiographs, CT scan, technetium bone scan, or MRI. Athletes with this injury typically present with dull to progressively sharp anterior chest pain. In addition to weightlifting, stress fractures of the sternum have also been described in athletes participating in golf [19] and wrestling [20]. In one case described in the literature, the athlete described an audible “pop” [21] while performing core exercises for the abdominal muscles during training. In all cases of sternal stress fractures described in the literature, the athletes were performing intensified repetitive activities of the pectoralis muscles or rectus abdominis in preparation for competitions. Relative rest from the causative activity led to resolution of symptoms within 6–10 weeks.
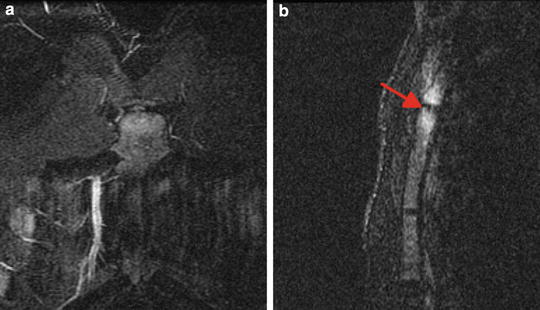
Fig. 14.4
T2 coronal (a) and sagittal (b) MRI series demonstrating stress fracture of the mid sternum in a competitive weight lifter
Scapula
Stress fractures of the scapula in athletes are uncommon [22, 23]. Cases reported in the literature include a gymnast, a baseball pitcher, a jogger carrying weights, and a professional football player [4, 10, 22, 24]. Additional cases have included stress fractures of the dominant shoulder in the scapular spine of a high school football quarterback (Fig. 14.5) and a trap shooter with a coracoid stress fracture [25] and an athlete undergoing shoulder rehabilitation following shoulder surgery. Scapular sites where stress fractures have been diagnosed include the coracoid, acromion (Fig. 14.6), scapular spine, and scapular body [10, 22, 26]. Given that the scapula has a complex array of muscle attachments and corresponding bone stress patterns, these injuries represent a diagnostic challenge to clinicians. Depending on the motion, stress concentration occurs at a variety of locations in the scapula. Authors have theorized that the likely cause of these injuries is overuse or fatigue of one or more of the 17 muscles that control the scapula, leading to stress-related injury [4, 7, 10].
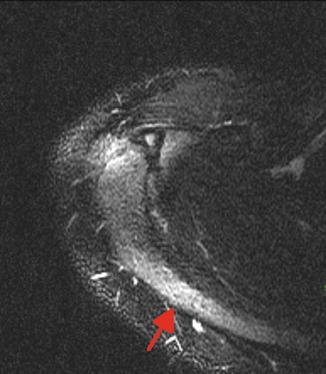
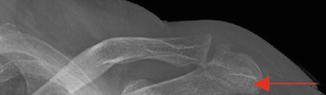
Fig. 14.5
T2 axial MRI demonstrating Grade 2 stress fracture of the medial scapular spine in the dominant right shoulder of a high school quarterback. An unstable os acromiale is also evident
Fig. 14.6
Anteroposterior radiographs of the left shoulder demonstrating Grade 3 stress fracture of the acromion process
Clavicle
Reports of clavicular stress fractures have involved athletic activities such as rowing, diving, javelin, weightlifting, gymnastics, and baseball [4, 6, 23]. Abnormal bending, shear, and rotational forces can develop across the clavicle if there is any imbalance in muscular contraction between the pectoralis major, deltoid, and sternocleidomastoid muscles [4]. Repetitive bone strain by these forces may exceed the reparative capacity of the bone and lead to a stress fracture. Seyahi et al. [23] described a patient with a clavicular stress fracture presenting as atypical severe arm pain radiating throughout the upper extremity and hemithorax. In the case of clavicular stress fractures, activity modification until pain is resolved, postural training, and scapulothoracic stabilization exercises have yielded symptom resolution [4, 23].
Proximal Humerus
Stress fractures of the proximal humerus have been described most commonly in throwing and overhead athletes and weight lifters [27–30]. In throwers and overhead athletes such as tennis players, poor conditioning and fatigue of the shoulder girdle musculature allows for increased rotational strain at the cortical surface predisposing to stress fracture. Bending forces generated by opposition of the deltoid and pectoralis major muscles is the suspected mechanism for the transversely oriented stress fractures in weight lifters [31]. Athletes either present with increasing arm pain of an insidious onset or acute on chronic pain or a “pop” following antecedent activity related pain of the shoulder or arm [4].
If incomplete or non-displaced, proximal humeral stress fractures may be treated nonoperatively in a sling or fracture brace until the athlete is pain-free with activities of daily living or radiographic healing is evident. Treatment for incomplete or non-displaced proximal humeral stress fractures should also include rest and cessation of the offending activity. However, 12 months may be required for the patient to become asymptomatic [10]. If there is displacement, open reduction and internal fixation may be necessary to ensure timely healing.
Little League Shoulder
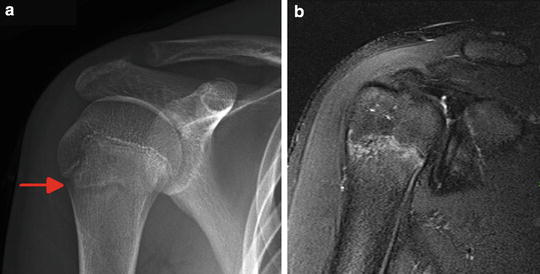
Little League shoulder is epiphysiolysis of the proximal humerus secondary to repetitive microtrauma from overhead activity [32]. The proximal humeral physis fuses approximately between the ages of 14 and 17 years in females and between 16 and 18 years in males [33, 34]. Factors that contribute to the development of Little League shoulder include excessive throwing, poor technique, and muscular imbalance. Athletes typically describe diffuse shoulder pain that is worse with throwing often following an increase in the throwing frequency or intensity [35–37]. On physical examination patients demonstrate weakness with resisted abduction and internal rotation along with tenderness and swelling over the anterolateral shoulder.
Anteroposterior X-rays may reveal widening of the proximal humeral physis (Fig. 14.7a). Plain radiographs may also display fragmentation or demineralization of the metaphysis and periosteal reaction.[35–37] MRI of the shoulder may be required if the diagnosis is unclear (Fig. 14.7b). Treatment requires rest from throwing for 6–12 weeks followed by a progressive throwing program with alterations of throwing techniques and biomechanics as needed. The return to throwing progression begins with light tossing and gradual progression with increasing distance and velocity [35]. Potential complications of this injury include premature physeal closure with resultant humeral length discrepancy or angular deformity although with the great remodeling potential of the proximal humerus, these complications are rare. Proper throwing mechanics and close monitoring of the number of pitches thrown by a skeletally immature athlete are crucial for recovery from little league shoulder and prevention of further injury.