Chapter 4 SECTION 2 THIGH, HIP, AND PELVIS SECTION 3 LEG, FOOT, AND ANKLE V. Impingement Syndrome/Rotator Cuff Disease VI. Superior Labral and Biceps Tendon Injuries VII. Acromioclavicular and Sternoclavicular Injuries IX. Calcifying Tendinitis and Shoulder Stiffness SECTION 8 MEDICAL ASPECTS OF SPORTS MEDICINE I. Preparticipation Physical Examination IV. Delayed-Onset Muscle Soreness V. Cardiac Abnormalities in Athletes VI. Metabolic Issues in Athletes VIII. Female Athlete–Related Issues 1. Hinge joint that also incorporates both gliding and rolling, which are essential to its kinematics 2. See Chapter 2, Anatomy, for a thorough discussion of knee anatomy. 4. Medial structures of the knee (three layers) (Table 4-1; Figure 4-2) Table 4-1 MCL, medial collateral ligament. Note: The gracilis, semitendinosus, and saphenous nerves run between layers I and II. 5. Lateral structures of the knee (three layers) (Table 4-2; see Figure 4-2) Table 4-2 Lateral Structures of the Knee LCL, lateral collateral ligament. 1. Ligamentous biomechanics: The role of the ligaments of the knee is to provide passive restraints against abnormal motion (Table 4-3). Table 4-3 Biomechanics of Knee Ligaments 2. Structural properties of ligaments: The tensile strength of a ligament, or maximal stress that a ligament can sustain before failure, has been characterized for all knee ligaments. However, it is important to consider age, ligament orientation, preparation of the specimen, and other factors before determining which graft to use. 3. Kinematics: The motion of the knee joint and interplay of ligaments have been described as a four-bar cruciate linkage system (Figure 4-5). 1. Complete history of the injury 2. Clarification of mechanism of injury 4. Important key historical points (Table 4-4) Table 4-4 Key Historical Points That Indicate Mechanism of Injury ACL, anterior cruciate ligament; PCL, posterior cruciate ligament. 1. Key examination points are shown in Table 4-5. Table 4-5 2. Examination performed with the patient under anesthesia may be helpful in some cases. C Instrumented measurement of knee laxity 1. KT-1000 and KT-2000 Knee Ligament Arthrometers (MEDmetric, San Diego, California) are the devices most commonly used for standardized laxity measurement. Table 4-6 Knee Injuries: Radiographic Findings 2. Stress radiographs: These are useful for evaluating injuries to the femoral physis (to differentiate from MCL injury) and are becoming the “gold standard” in diagnosing and quantifying PCL injury. They can also be used to evaluate LCL and PLC injuries. 3. Nuclear imaging: Technetium-99m bone scans are useful in diagnosing stress fractures, early degenerative joint disease, and complex regional pain syndrome. 4. Magnetic resonance imaging (MRI): This has become the imaging modality of choice for diagnosis of ligament injuries, meniscal disease, avascular necrosis, spontaneous osteonecrosis of the knee, and articular cartilage defects and has replaced the use of arthrography. On coronal MRI sequences, meniscal root tears are seen as a band of low-signal fibrocartilage. Occult fractures of the knee can be identified by a double fluid-fluid layer, which signifies lipohemarthrosis. 5. Magnetic resonance arthrography: Intraarticular magnetic resonance arthrography is the most accurate imaging method for confirming the diagnosis of repeated meniscal tears after repair. 6. Computed tomography (CT): CT has been replaced largely by MRI, but it is still useful in the evaluation of bony tumors, patellar tilt, and fractures. CT has been advocated as a tool to assist in operative planning for patellar realignment by allowing measurement of the tibial tuberosity–trochlear groove (TT-TG) distance; authors recommend distal realignment procedures for a TT-TG distance exceeding 20 mm. MRI can also be used to measure TT-TG distance. 7. Arthrography: This technique was useful historically for the diagnosis of MCL tears and has been supplanted by MRI. However, it can be useful when MRI is not available or tolerated by the patient, and it can be combined with CT. 8. Tomography: Tomograms are preferred to CT in the evaluation of tibial plateau fractures at some medical centers. 9. Ultrasonography: This technique is useful for detecting soft tissue lesions about the knee, including patellar tendinitis, hematomas, and extensor mechanism ruptures, in some centers. Ultrasonography has begun to be used to evaluate meniscal tears but is not as sensitive as MRI. E Arthrocentesis and intraarticular knee injection See Supplemental Images on expertconsult.com. 1. The “gold standard” for the diagnosis of knee disease 2. The benefits of arthroscopic over open techniques include smaller incisions, less morbidity, improved visualization, and decreased recovery time. 2. Accessory portals, sometimes helpful for visualizing the posterior horns of the menisci and PCL 1. Each knee arthroscopy should include an evaluation of the suprapatellar pouch; patellofemoral joint and tracking; medial and lateral gutters; medial compartment, including the medial meniscus and the articular surface; the lateral compartment, including the lateral meniscus and the articular surface; and the intercondylar notch to visualize the ACL and PCL. 2. The posteromedial corner can be best visualized with a 70-degree arthroscope placed through the notch (modified Gillquist view) or a posteromedial portal.
Sports Medicine
section 1 Knee
 Anterior cruciate ligament (ACL)
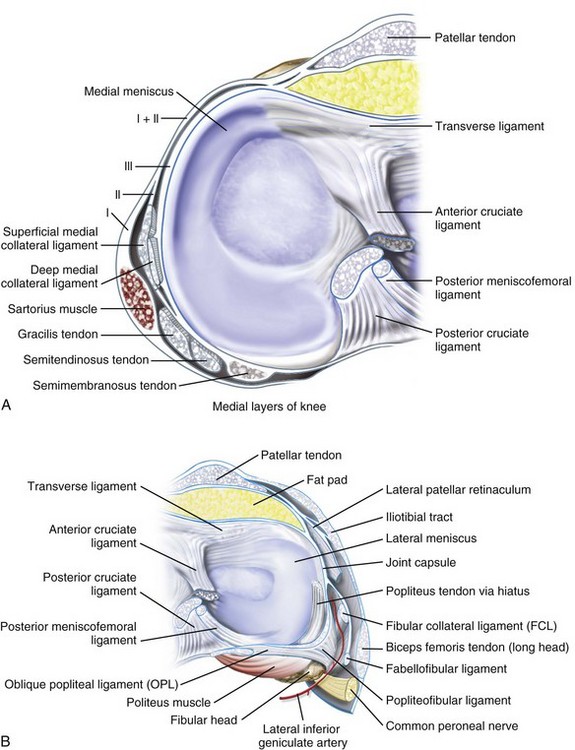
Anterior cruciate ligament (ACL)
 Despite intensive research, the function and anatomy of the ACL are still debated.
Despite intensive research, the function and anatomy of the ACL are still debated.
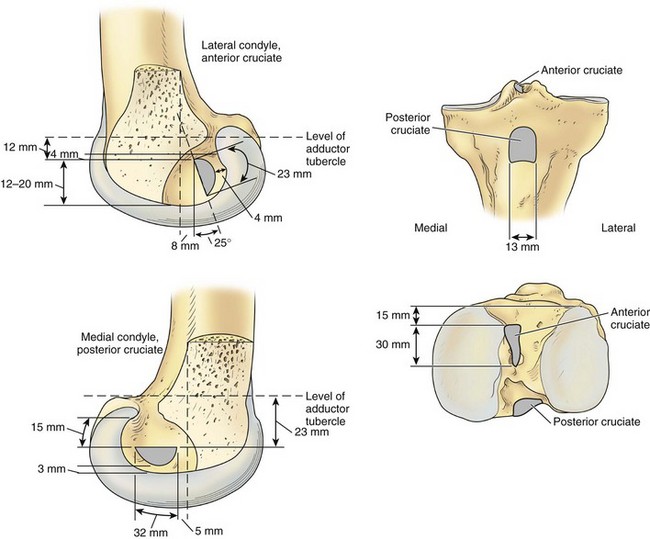
 Femoral attachment: semicircular area on the posteromedial aspect of the lateral femoral condyle (Figure 4-1)
Femoral attachment: semicircular area on the posteromedial aspect of the lateral femoral condyle (Figure 4-1)
 Has two “bundles” named on the basis of tibial insertion:
Has two “bundles” named on the basis of tibial insertion:
 Anteromedial: tight in flexion; primarily an anterior restraint; evaluated by Lachman and anterior drawer tests
Anteromedial: tight in flexion; primarily an anterior restraint; evaluated by Lachman and anterior drawer tests
 Posterolateral: tight in extension; primarily a rotatory restraint; evaluated by pivot shift test
Posterolateral: tight in extension; primarily a rotatory restraint; evaluated by pivot shift test
 Composition: 90% type I collagen and 10% type III collagen
Composition: 90% type I collagen and 10% type III collagen
 Mechanoreceptor nerve fibers within the ACL have been found and may have a proprioceptive role.
Mechanoreceptor nerve fibers within the ACL have been found and may have a proprioceptive role.
 Posterior cruciate ligament (PCL)
Posterior cruciate ligament (PCL)
 Femoral attachment: broad, crescent-shaped area on the anterolateral medial femoral condyle
Femoral attachment: broad, crescent-shaped area on the anterolateral medial femoral condyle
 Tibial insertion: tibial sulcus below articular surface (see Figure 4-1)
Tibial insertion: tibial sulcus below articular surface (see Figure 4-1)
 Medial collateral ligament (MCL)
Medial collateral ligament (MCL)
 Superficial MCL (tibial collateral ligament)
Superficial MCL (tibial collateral ligament)
 Lies deep to the gracilis and semitendinosus tendons
Lies deep to the gracilis and semitendinosus tendons
 Originates 3.2 mm proximal and 4.8 mm posterior from the medial femoral epicondyle
Originates 3.2 mm proximal and 4.8 mm posterior from the medial femoral epicondyle
 Inserts onto the periosteum of the proximal tibia, deep to the pes anserinus
Inserts onto the periosteum of the proximal tibia, deep to the pes anserinus
 Superficial fibers insert 61.2 mm distal to the knee joint.
Superficial fibers insert 61.2 mm distal to the knee joint.
 Deep portion of the ligament (medial capsular ligament)
Deep portion of the ligament (medial capsular ligament)
 Lateral collateral ligament (LCL); also known as the fibular collateral ligament
Lateral collateral ligament (LCL); also known as the fibular collateral ligament
 Origin: lateral femoral epicondyle
Origin: lateral femoral epicondyle
 Insertion: anterolateral aspect of the fibular head
Insertion: anterolateral aspect of the fibular head
 Tight in extension and lax in flexion because of its location behind the axis of knee rotation
Tight in extension and lax in flexion because of its location behind the axis of knee rotation
 Deep and posterior to the superficial MCL, contiguous with the deep MCL
Deep and posterior to the superficial MCL, contiguous with the deep MCL
 Important factor in rotary stability
Important factor in rotary stability
 The posteromedial corner has three components:
The posteromedial corner has three components:
 Increasingly important factor in the treatment of the multiple ligament injured knee
Increasingly important factor in the treatment of the multiple ligament injured knee
 Originates on the back of the tibia
Originates on the back of the tibia
 The femoral insertion is inferior, anterior, and deep to the LCL.
The femoral insertion is inferior, anterior, and deep to the LCL.
 Arcuate ligament (which is contiguous with the oblique popliteal ligament medially)
Arcuate ligament (which is contiguous with the oblique popliteal ligament medially)
 Fabellofibular ligament (lateral two are really just thickenings of the joint capsule)
Fabellofibular ligament (lateral two are really just thickenings of the joint capsule)
 The PLC is the primary stabilizer of external tibial rotation.
The PLC is the primary stabilizer of external tibial rotation.
Layer
Components
I
Sartorius and fascia
II
Superficial MCL, posterior oblique ligament, semimembranosus
III
Deep MCL, capsule
Layer
Components
I
Iliotibial tract, biceps, fascia
II
Patellar retinaculum, patellofemoral ligament
III
Arcuate ligament, fabellofibular ligament, capsule, LCL
 The order of insertion of structures on the proximal fibula is, from anterior to posterior, the LCL, the popliteofibular ligament, and the biceps femoris.
The order of insertion of structures on the proximal fibula is, from anterior to posterior, the LCL, the popliteofibular ligament, and the biceps femoris.
 Crescent-shaped, fibrocartilagenous structures
Crescent-shaped, fibrocartilagenous structures
 Composed predominantly of type 1 collagen
Composed predominantly of type 1 collagen
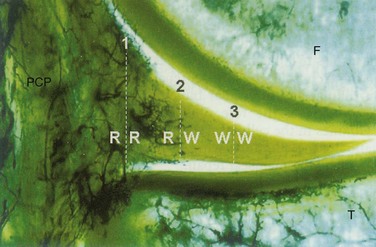
 Only the peripheral 20% to 30% of the medial meniscus and the peripheral 10% to 25% of the lateral meniscus are vascularized (medial and lateral genicular arteries, respectively; see Figure 4-1).
Only the peripheral 20% to 30% of the medial meniscus and the peripheral 10% to 25% of the lateral meniscus are vascularized (medial and lateral genicular arteries, respectively; see Figure 4-1).
 Medial meniscus is more C-shaped; lateral meniscus is more circular (see Figure 4-1).
Medial meniscus is more C-shaped; lateral meniscus is more circular (see Figure 4-1).
 The two menisci are connected anteriorly by the transverse (intermeniscal) ligament.
The two menisci are connected anteriorly by the transverse (intermeniscal) ligament.
 They are attached peripherally by coronary ligaments.
They are attached peripherally by coronary ligaments.
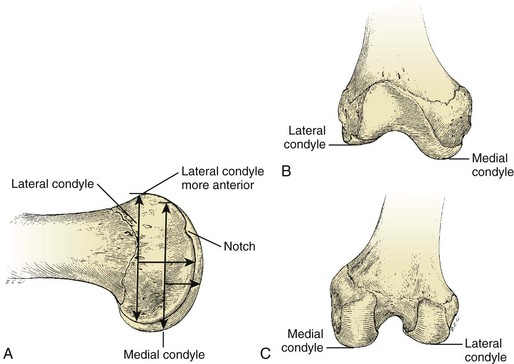
 Greater anteroposterior dimensions than medial condyle
Greater anteroposterior dimensions than medial condyle
 Relatively straight in comparison with medial condyle
Relatively straight in comparison with medial condyle
 Has a terminal sulcus and a groove of the popliteus insertion (Figure 4-3)
Has a terminal sulcus and a groove of the popliteus insertion (Figure 4-3)
 Articulation between the patella and femoral trochlea
Articulation between the patella and femoral trochlea
 Patella has variably sized medial and lateral facets.
Patella has variably sized medial and lateral facets.
 Articular surface of the patella is the thickest in the body.
Articular surface of the patella is the thickest in the body.
 The patella can withstand forces several times those of body weight.
The patella can withstand forces several times those of body weight.
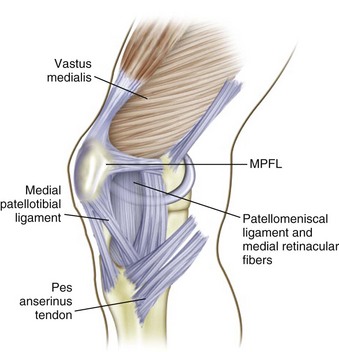
 The medial patellofemoral ligament is present in the second medial layer (Figure 4-4).
The medial patellofemoral ligament is present in the second medial layer (Figure 4-4).
Ligament
Restraint
ACL
Minimizing anterior translation of the tibia in relation to the femur (85%)
PCL
Minimizing posterior tibial displacement (95%)
MCL
Minimizing valgus angulation
LCL
Minimizing varus angulation
MCL and LCL
Acting in concert with posterior structures to control axial rotation of the tibia on the femur
PCL and posterolateral corner
Acting synergistically to resist posterior translation and posterolateral rotary instability
 ACL: approximately 2200 N and up to 2500 N in young individuals
ACL: approximately 2200 N and up to 2500 N in young individuals
 The tensile strength of a 10-mm patellar tendon graft (young specimen) is more than 2900 N and is about 30% stronger when it is rotated 90 degrees. However, this strength quickly diminishes in vivo.
The tensile strength of a 10-mm patellar tendon graft (young specimen) is more than 2900 N and is about 30% stronger when it is rotated 90 degrees. However, this strength quickly diminishes in vivo.
 PCL: approximately 2500 to 3000 N, but this has been disputed
PCL: approximately 2500 to 3000 N, but this has been disputed
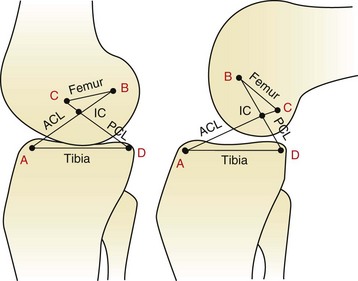
 As the knee flexes, the center of joint rotation (intersection of the cruciate ligaments) moves posteriorly, causing rolling and gliding at the articulating surfaces.
As the knee flexes, the center of joint rotation (intersection of the cruciate ligaments) moves posteriorly, causing rolling and gliding at the articulating surfaces.
 The concept of ligament “isometry” remains controversial.
The concept of ligament “isometry” remains controversial.
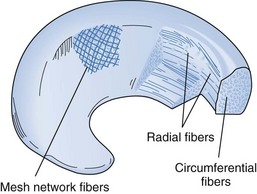
 The collagen fibers of the menisci are arranged radially and longitudinally (Figure 4-6).
The collagen fibers of the menisci are arranged radially and longitudinally (Figure 4-6).
 Studies have shown that an ACL deficiency may result in abnormal meniscal strain, particularly in the posterior horn of the medial meniscus (Figure 4-7).
Studies have shown that an ACL deficiency may result in abnormal meniscal strain, particularly in the posterior horn of the medial meniscus (Figure 4-7).

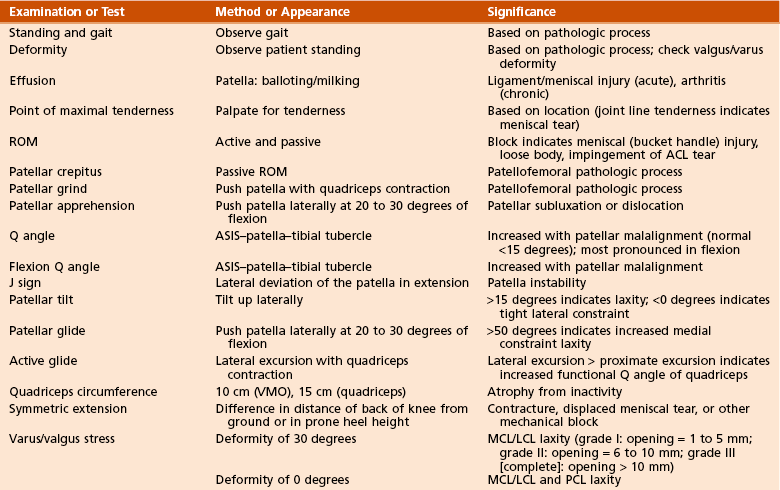
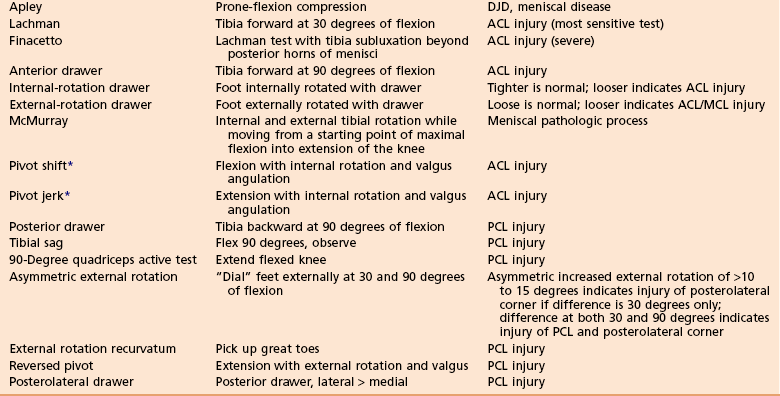
History
Significance
Pain after sitting or climbing stairs
Patellofemoral cause
Locking or pain with squatting
Meniscal tear
Noncontact injury with “popping” sound/sensation
ACL tear, patellar dislocation
Contact injury with “popping” sound
Collateral ligament tear, meniscal tear, fracture
Acute swelling
ACL tear, peripheral meniscal tear, osteochondral fracture, capsule tear
Knee “gives way”
Ligamentous laxity, patellar instability
Anterior force: dorsiflexed foot
Patellar injury
Anterior force: plantar-flexed foot
PCL injury
Dashboard injury
PCL or patellar injury
Hyperextension, varus angulation, and tibial external rotation
Posterolateral corner injury

 Most common causes of an acute hemarthrosis: ACL tear (70%), patella dislocation, osteochondral fracture, and isolated meniscal tear
Most common causes of an acute hemarthrosis: ACL tear (70%), patella dislocation, osteochondral fracture, and isolated meniscal tear
 Weight-bearing 45-degree posteroanterior view
Weight-bearing 45-degree posteroanterior view
 Merchant or Laurin view of the patella
Merchant or Laurin view of the patella
 Several findings and their significance are listed in Table 4-6.
Several findings and their significance are listed in Table 4-6.

View/Sign
Findings
Significance
Lateral-high patella
Patella alta
Patellofemoral pathologic process
Congruence angle
µ = −6 degrees; SD = 11 degrees
Patellofemoral pathologic process
Tooth sign
Irregular anterior patella
Patellofemoral chondrosis
Varus/valgus stress view
Opening
Collateral ligament injury; Salter-Harris fracture
Lateral capsule (Segond) sign
Small tibial avulsion off lateral tibia
ACL tear
Pellegrini-Stieda lesion
Avulsion of medial femoral condyle
Chronic MCL injury
Lateral-stress view: stress to anterior tibia with knee flexed 70 degrees
Asymmetric posterior tibial displacement
PCL injury
Weight-bearing posteroanterior view flexion
Early DJD, OCD, notch evaluation
Fairbank changes
Square condyle, peak eminences, ridging, narrowing
Early DJD (postmeniscectomy)
Square lateral condyle
Thickened joint space
Discoid meniscus
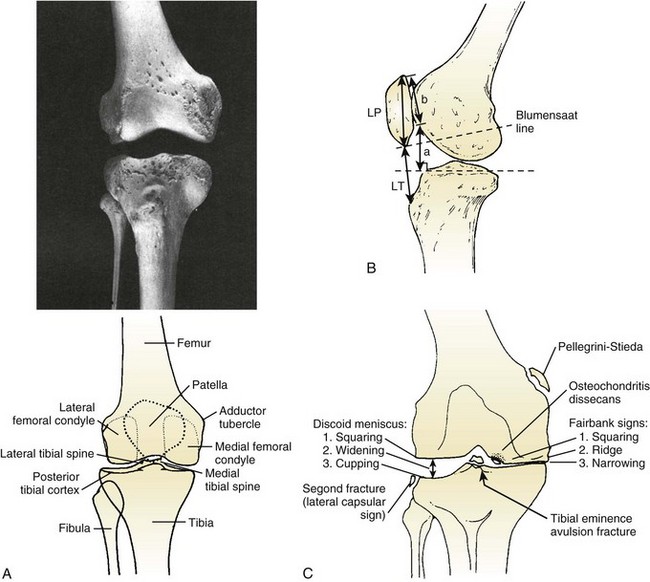
 Normal bony anatomy is demonstrated in Figure 4-8, A. Many of these findings are illustrated in Figure 4-8, B.
Normal bony anatomy is demonstrated in Figure 4-8, A. Many of these findings are illustrated in Figure 4-8, B.
 Evaluation of patella height is accomplished by one of three commonly used methods (see Figure 4-8, C).
Evaluation of patella height is accomplished by one of three commonly used methods (see Figure 4-8, C).
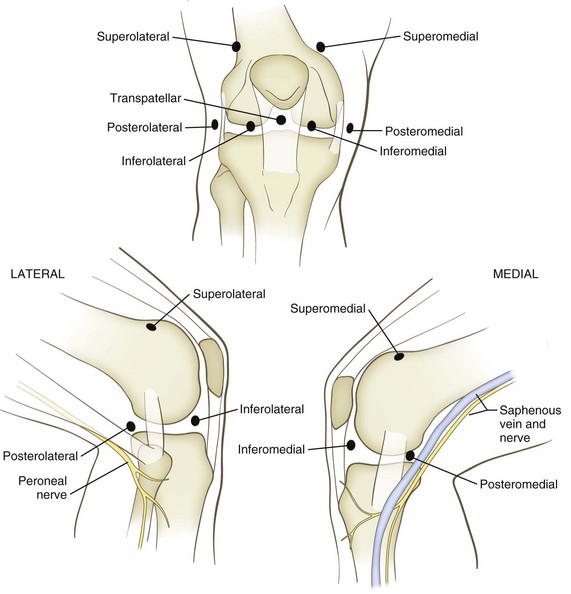
 Posteromedial portal: 1 cm above the joint line behind the MCL (be careful to avoid saphenous nerve branches)
Posteromedial portal: 1 cm above the joint line behind the MCL (be careful to avoid saphenous nerve branches)
 Meniscal tears are the most common injury to the knee that necessitates surgery.
Meniscal tears are the most common injury to the knee that necessitates surgery.
 The medial meniscus is torn approximately three times more often than the lateral meniscus.
The medial meniscus is torn approximately three times more often than the lateral meniscus.
 There is an increased rate of osteoarthritis in knees after both meniscal tears and meniscectomy.
There is an increased rate of osteoarthritis in knees after both meniscal tears and meniscectomy.
 Traumatic meniscal tears are common in young patients with sports-related injuries.
Traumatic meniscal tears are common in young patients with sports-related injuries.
 Degenerative tears usually occur in older patients and can have an insidious onset.
Degenerative tears usually occur in older patients and can have an insidious onset.
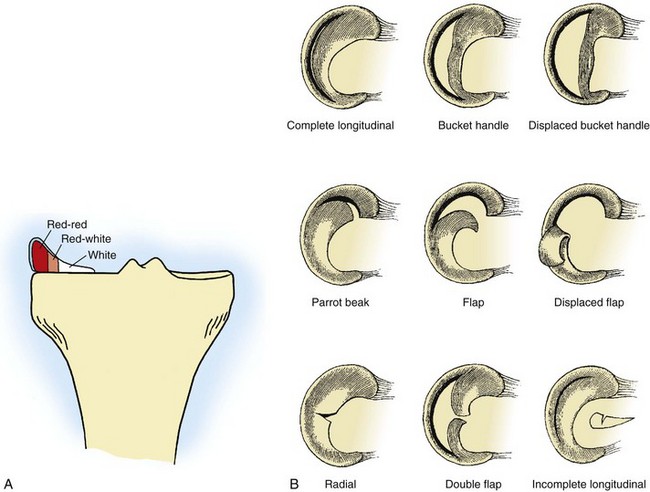
 Meniscal tears can be classified according to their location in relation to the vascular supply, their position (anterior, middle, or posterior third), and their appearance and orientation (Figure 4-10).
Meniscal tears can be classified according to their location in relation to the vascular supply, their position (anterior, middle, or posterior third), and their appearance and orientation (Figure 4-10).
 Meniscal root tears completely disrupt the circumferential fibers of the meniscus and can lead to meniscal extrusion.
Meniscal root tears completely disrupt the circumferential fibers of the meniscus and can lead to meniscal extrusion.
 The vascular supply of the meniscus is a primary determinant of healing potential.
The vascular supply of the meniscus is a primary determinant of healing potential.
 In the absence of intermittent swelling, catching, locking, or giving way, meniscal tears—particularly those degenerative in nature—may be treated conservatively.
In the absence of intermittent swelling, catching, locking, or giving way, meniscal tears—particularly those degenerative in nature—may be treated conservatively.
 Tears that are not amenable to repair (e.g., peripheral, longitudinal tears)—excluding those that do not necessitate any treatment (e.g., partial-thickness tears, those <5 to 10 mm in length, and those that cannot be displaced >1 to 2 mm)—are best treated by partial meniscectomy.
Tears that are not amenable to repair (e.g., peripheral, longitudinal tears)—excluding those that do not necessitate any treatment (e.g., partial-thickness tears, those <5 to 10 mm in length, and those that cannot be displaced >1 to 2 mm)—are best treated by partial meniscectomy.
 Should be done for all peripheral longitudinal tears, especially in young patients and in conjunction with an ACL reconstruction
Should be done for all peripheral longitudinal tears, especially in young patients and in conjunction with an ACL reconstruction
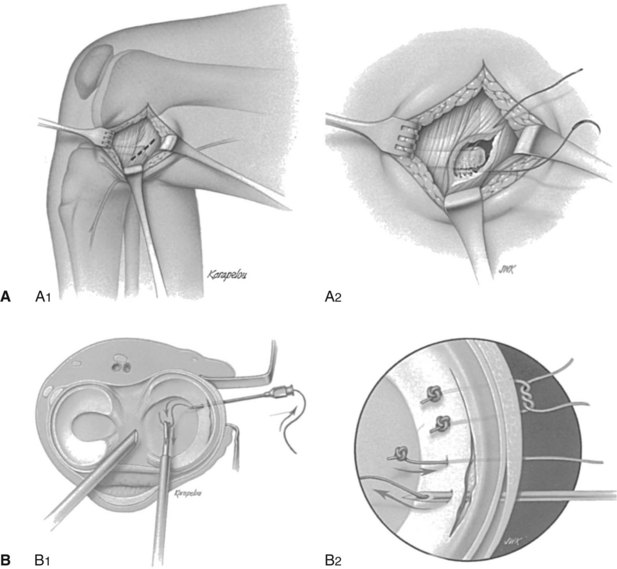
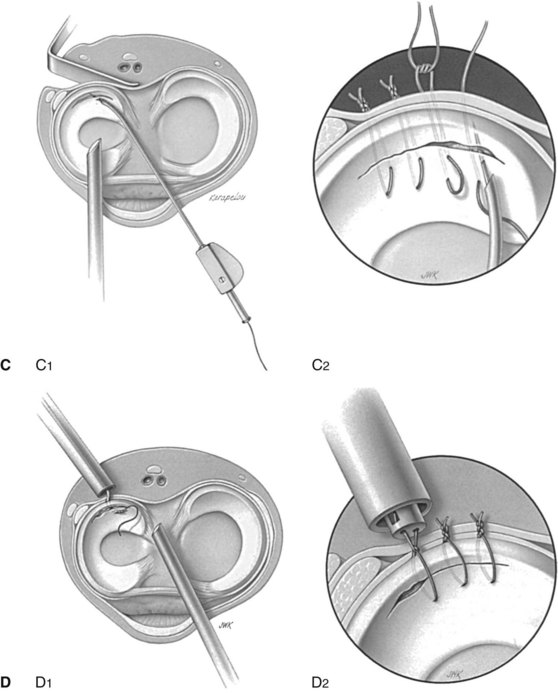
 Four techniques are commonly used: open, “outside-in,” “inside-out,” and “all-inside” (Figure 4-12).
Four techniques are commonly used: open, “outside-in,” “inside-out,” and “all-inside” (Figure 4-12).
 The latest generation of “all-inside” devices allows tensioning of the construct.
The latest generation of “all-inside” devices allows tensioning of the construct.
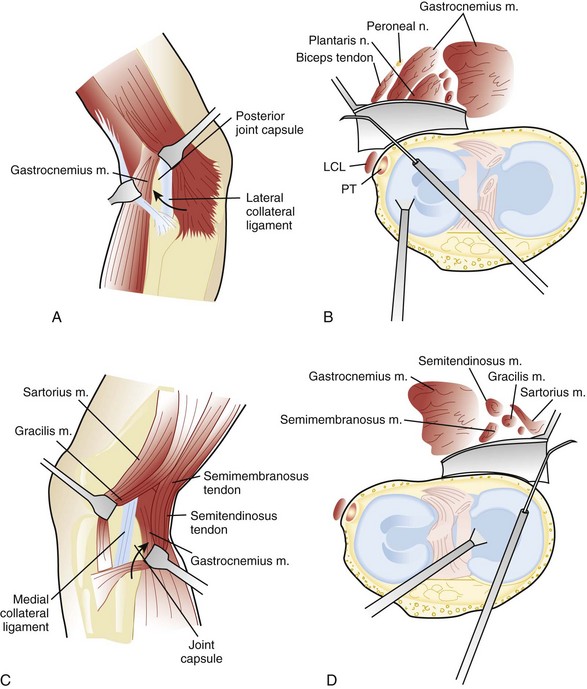
 Regardless of the technique used, it is essential to protect the saphenous nerve branches (anterior to both the semitendinosis and gracilis muscles and posterior to the inferior border of the sartorius muscle) during medial repairs and to protect the peroneal nerve (posterior to the biceps femoris) during lateral repairs (Figure 4-13).
Regardless of the technique used, it is essential to protect the saphenous nerve branches (anterior to both the semitendinosis and gracilis muscles and posterior to the inferior border of the sartorius muscle) during medial repairs and to protect the peroneal nerve (posterior to the biceps femoris) during lateral repairs (Figure 4-13).