4 Spinal positioning and locking
Note: Principles of spinal positioning locking on the DVD-ROM should be viewed in conjunction with Chapter 4.
Spinal Locking
Spinal locking is necessary for long-lever high-velocity low-amplitude (HVLA) thrust techniques to localize forces and achieve cavitation at a specific vertebral segment.1–7 Short-lever HVLA thrust techniques do not require locking of adjacent spinal segments.
Locking can be achieved by either facet apposition or the utilization of ligamentous myofascial tension, or a combination of both.1–57 The principle used in these approaches is to position the spine in such a way that leverage is localized to one joint without undue strain being placed upon adjacent segments.
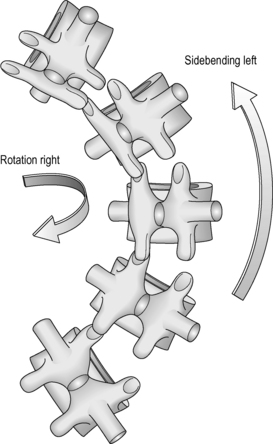
• Type 1 movement – sidebending and rotation occur in opposite directions (Fig. 4.18)
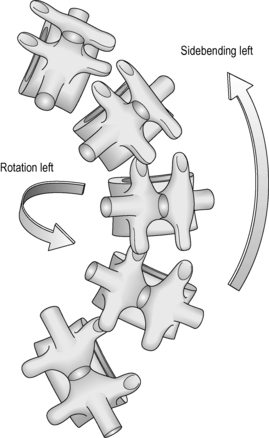
• Type 2 movement – sidebending and rotation occur in the same direction (Fig. 4.28).
Spinal Positioning
Cervical spine
A number of authors describe the normal coupling at the occipito-atlantal (C0–1) segment as axial rotation and lateral bending to the opposite side (i.e. Type 1 movement).7,9,10 The principle of facet apposition locking does not apply to HVLA thrust techniques directed to the C0–1 segment. However, facet apposition locking of the C0–1 segment can be utilized for HVLA thrust techniques directed to other cervical levels (Table 4.1).
| Spinal level | Coupled motion | Facet apposition locking |
|---|---|---|
| C0–1 (occipito-atlantal) | Type 1 | Type 2 |
| C1–2 (atlanto-axial) | Complex-primary rotation | Not Applicable |
| C2–7 | Type 2 | Type 1 |
The type of coupled movement available at the C1–2 segment is complex. This segment has a predominant role in total cervical rotation.11–14 Up to 77% of total cervical rotation occurs at the atlanto-axial joint, with a mean rotation range of 40.5° to either side.11,13 The great range of rotation at the atlanto-axial joint can be attributed to facet plane, the loose nature of the ligamentous fibrous capsule and the absence of ligamentum flavum above C2.14 Only a small amount of rotation occurs at the joints above and below the atlanto-axial joint.15–17
Below C2, normal coupling behaviour in the cervical spine is Type 2 (i.e. sidebending and rotation occur to the same side).7,9,18–22 The average range of cervical spine rotation from neutral position is 80° (Fig. 4.3).23 For patient comfort and safety the practitioner should limit the total range of cervical spine rotation when applying thrust techniques. Below C2 this is achieved by combining cervical spine rotation with opposite sidebending (Fig. 4.4). To generate facet apposition locking for HVLA thrust techniques, the operator must introduce a Type 1 movement, which is sidebending of the cervical spine in one direction and rotation in the opposite direction (e.g. sidebending right with rotation left). This positioning locks the segments above the joint to be cavitated and enables a thrust to be applied to one vertebral segment. The amount or degree of sidebending and rotation can be varied to obtain facet locking. The intent should be to have a primary and secondary leverage. The principal or primary leverage can be either sidebending or rotation (Fig. 4.5).


Figure 4.4 Introduction of right sidebending limits the range of available left cervical spine rotation.







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


