TABLE 26-1 Commonly Used Clinical Scales | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
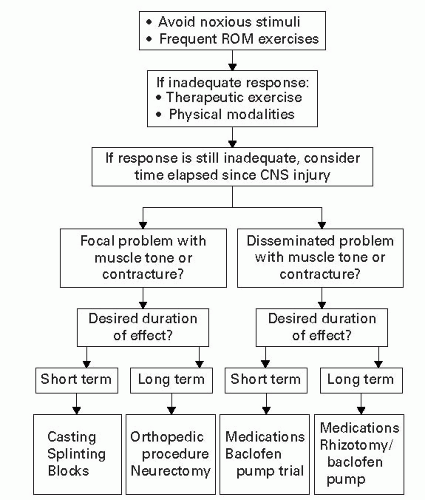 Figure 26-1 Algorithm for treating spasticity. Courtesy of Katz R. Spasticity. In: O’Young BJ, ed. Physical Medicine & Rehabilitation Secrets. 2nd ed. Philadelphia, PA: Hanley & Belfus; 2002:144. |
to skin breakdown. Cryotherapy (>15 minutes) may be helpful transiently by reducing the hyperexcitability of the muscle stretch reflex and reducing nerve conduction velocities. Functional electrical stimulation (>15 minutes) can improve function and reduce tone for hours after the stimulation (thought to be due to neurotransmitter modulation at the spinal cord level). Hippotherapy, which involves rhythmic movements, is found useful in spasticity reduction in lower limbs. Other modalities include application of tendon pressure, cold, warmth, vibration, massage, low-power laser, and acupuncture.1
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


