Indications
Contraindications
Fall on outstretched hand
Compound fractures
Tenderness at anatomic snuffbox
Displaced fractures
Ulnar collateral ligament injury of the thumb (Gamekeeper’s thumb)
Multiple trauma
DeQuervain’s tenosynovitis
Open wound
Nondisplaced distal radius fractures
The inability to have the patient come in for proper follow-up
The inability of the patient to follow instructions (developmentally disabled, child)
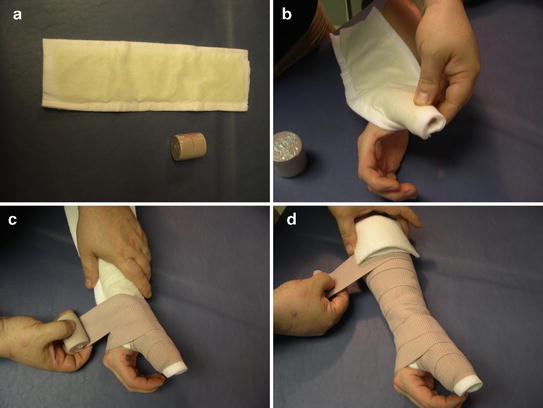
Fig. 15.1
Thumb spica splint. (a) Two or four inch prepackaged splint material (padding included) and a 2 in. ace wrap. (b) Padded side of splint applied facing toward the patient. Fold splint around distal thumb. Immobilize MP joint. (c) Wrap with 2 in. ace; overlap by one-half inch with slight tension. Do not over tighten. Notice how to efficiently wrap spica by unwrapping ace in a counterclockwise direction. (d) Fold proximal aspect of splint material so splint only covers three-quarters of forearm and does not impinge upon the antecubital fossa
The patient should be seated in a comfortable position with the affected extremity supported. The hand should be held in the “safe hand” position (see Fig. 5.6). The thumb is not placed in anatomic position or abducted in the “hitch hiker” position. The patient can be instructed to hold the hand as if holding a “favorite cold beverage” to demonstrate the safe hand position. The splint can be applied using stockinette, then cast padding, then tape. A splint material that has everything integrated is also available. This is the author’s preferred method. The splint material is first placed in water. (If the water is hot, the casting tape will set up prematurely. If the water is cold, the casting tape may take up to 45 min to set.) The splint is folded around the distal part of the thumb. The MP joint is immobilized. The elastic bandage is overlapped by approximately one-half width and a very slight amount of tension is placed on the ace wrap. If too much tension is placed on the ace wrap, it will constrict the hand and the patient will complain of pain. The splint ends should cover approximately three-quarters of the forearm, and the excess casting padding should be folded back. The elastic bandage is wrapped until the splint is completely covered and the patient is held in a position of function until the material hardens (see Fig. 15.2). Proper instruction for care should be given to the patient. This splint may be removed when treating DeQuervain’s tenosynovitis or it may be kept in place until the patient has a follow-up. The splinting material should not be allowed to become wet and should be covered in plastic when bathing. Splints function well for 7–14 days and are not designed to be used for prolonged therapy. Depending upon the patient’s diagnoses, the splint may be replaced as many times as necessary at follow-up office visits.

Fig. 15.2
After the splint is applied, mold the splint to the MP joint of the thumb by applying pressure as shown. Keep wrist in neutral position. Patients have a tendency to flex wrist, which is not acceptable
Sugar Tong Splint (See Table 15.2 and Fig. 15.3a–d)
Table 15.2
Sugar tong splint
Indications | Contraindications |
|---|---|
Transport patients with fracture of elbow or radius | Compound fractures |
Short-term immobilization | Displaced fractures |
Nondisplaced elbow fractures | Multiple trauma |
Immobilization for treatment of distal radius fracture (some clinicians prefer thumb spica splint with use of arm sling) | Open wound |
The inability to have the patient come in for proper follow-up | |
The inability of the patient to follow instructions (developmentally disabled, child) |
Fig. 15.3
Sugar tong splint. (a) Two or four inch packaged splint material and a 2 and 4 in. ace wrap. Should be long enough to immobilize elbow to forearm twice. If splint is not long enough, use two shorter splints and overlap them. (b) This is the most important step. Immobilize the elbow in 90° flexion. The splint should immobilize the wrist but allow for at least 90° of flexion of the MP joints of the hand. The dorsal aspect of the splint may slightly overlap the MP joints. (c) Apply 4 in. ace wrap around elbow, overlapping by one-half inch, very slight tension. After 4 in. wrap in place, use 2 in. wrap to hold splint around the wrist. (d) Complete, proper application of upper extremity sugar tong splint. Elbow held at 90°, wrist complete extension and the patient should be able to flex MP joints 90°. Always use an arm sling with this splint (not shown here)
The sugar tong splint may be used to immobilize the elbow and the wrist. When applying a sugar tong splint, it is imperative that the MP joints are allowed to flex 90°. When the wrist is splinted, the palmar aspect of the splint should be a number of inches shorter than the dorsal aspect of the splint. Excess material at the palmar aspect of the hand can be folded to allow the metacarpal phalangeal joints to flex 90°. It is important to keep the patient in an anatomic position. The wrist should be in a neutral position. Extension as well as radial and ulnar deviation should be avoided.
Arm Sling (See Table 15.3)
Table 15.3
Arm sling
Indications | Contraindications |
|---|---|
AC separation | The patient should not be put in sling for prolonged periods without follow-up |
Fractured clavicle | Severe injury of the C-spine |
Nonsurgical treatment of rotator cuff injury | |
Treatment of patient recovering from a relocation of a dislocated shoulder |
The sling should fit comfortably over the back of the shoulder and should not be placed around the patient’s neck. The arm should rest comfortably at about breast level. The sling can be universal for both the right and left sides and can be modified for extra support. A large ace wrap could be wrapped around the arm and the chest to further immobilize the upper extremity. It is important to adjust the sling so the patient feels comfortable. The patient should be instructed to keep the wrist in neutral position. If the wrist is flexed, the median nerve may be compressed and the patient will complain of paresthesias.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


