Shoulder Arthritis and Arthroplasty
Melissa A. Wright, MD
Anand M. Murthi, MD, FAAOS
Dr. Wright or an immediate family member has received research or institutional support from Zimmer and serves as a board member, owner, officer, or committee member of American Shoulder and Elbow Surgeons. Dr. Murthi or an immediate family member has received royalties from Aevumed, DePuy, a Johnson & Johnson Company, Globus Medical, and Ignite Orthopaedics; serves as a paid consultant to or is an employee of Aevumed, DePuy, a Johnson & Johnson Company, Globus Medical, Ignite Orthopaedics, Immertec, WRS-Work Rehabilitation Solutions, and Zimmer; has stock or stock options held in Aevumed, Catalyst Orthoscience, Ignite Orthopaedics, and VTail; has received research or institutional support from Catalyst, Stryker, and Zimmer; and serves as a board member, owner, officer, or committee member of American Academy of Orthopaedic Surgeons, American Shoulder and Elbow Surgeons, Association of Clinical Elbow and Shoulder Surgeons, and MidAtlantic Shoulder and Elbow Society.
ABSTRACT
There are numerous causes and disease processes that lead to symptomatic degenerative joint disease about the shoulder. Common disorders include acromioclavicular joint arthritis, glenohumeral joint osteoarthritis, inflammatory arthritis, osteonecrosis, instability arthropathy, posttraumatic arthropathy, and rotator cuff arthropathy. Each disorder has characteristic presentations, examination findings, radiographic characteristics, and treatment strategies. The past decade has seen great strides in diagnostics, preoperative planning, and implant designs. With the increase in both anatomic and reverse shoulder replacement, care with surgical planning and indications will lead to fewer complications and better outcomes.
Keywords: acromioclavicular; arthroplasty; posttraumatic; rheumatoid; shoulder arthritis
Introduction
Shoulder reconstruction has advanced significantly over the past decade, with improved anatomic shoulder arthroplasty designs, the expanded use of reverse shoulder arthroplasty (RSA), and a better understanding of arthroplasty fixation and failure. Understanding the many etiologies of arthrosis about the shoulder helps the surgeon guide treatment and plan proper surgical approaches for good patient outcomes.
Arthritis of the Acromioclavicular Joint
Arthritis of the acromioclavicular (AC) joint is a common cause of anterior and superior shoulder pain and often exists in conjunction with other shoulder pathology. Radiographic changes do not always correlate with clinical symptomatology, and the symptoms of AC joint arthritis are largely nonspecific. Incidentally identified AC joint arthritis does not require treatment. A 2019 study of 114 patients with degenerative changes of the AC joint on MRI found that 90% remained asymptomatic over 7 years.1 A careful physical examination including visual inspection, palpation, and provocative maneuvers alone can help identify clinically relevant AC joint arthritis. The cross-body adduction stress test is the most sensitive for AC joint arthritis (77%), whereas the O’Brien active compression test is most specific (95%).2 Radiographic imaging is sufficient to diagnose AC joint arthritis. The joint can be visualized on chest radiographs and standard shoulder radiographs. However, the AC joint is best visualized on the Zanca view (10° to 15° cephalad tilt and 50% penetration).3
For symptomatic AC joint arthritis, treatment begins with nonsurgical modalities such as activity modification, NSAIDs, and cortisone injections. A 2021 scoping review attempted to compare differences in outcome after surgical and nonsurgical management of AC joint arthritis and found no comparative studies. Fifteen studies of surgical management and four of nonsurgical management found improvement in patient-reported outcomes, with low complication rates across all studies.4
Surgical intervention for symptomatic AC joint arthritis involves distal clavicle excision (DCE), which can be performed arthroscopically or open. A systematic review of 17 studies comparing open versus arthroscopic DCE found no difference in patient-reported outcome scores, with possible faster return to activities after arthroscopic DCE if performed in isolation.5 The goal of DCE is to remove the pathology while minimizing destruction of the joint capsule and risk of instability. Safe resection length varies based on the individual, but should be less than 10 mm. Persistent pain, the most common complication after DCE, can be related to either inadequate resection or overresection and subsequent instability.
DCE is often performed in conjunction with rotator cuff repair (RCR). A systematic review evaluated patients undergoing arthroscopic RCR with and without DCE and found no difference in patient-reported outcomes, range of motion, pain, or repeat surgery between the groups.6 Additionally, there is low risk (1.1%) of repeat surgery to perform DCE after RCR if not performed initially, and therefore routine DCE is not recommended with RCR unless the patient is specifically symptomatic at the AC joint.7
Arthritis of the Glenohumeral Joint
Numerous disease processes and injury patterns can result in a degenerative glenohumeral joint. The most common disorders include osteoarthritis, inflammatory arthritis, osteonecrosis, rotator cuff arthropathy (RCA), posttraumatic arthritis, and postcapsulorrhaphy arthropathy. Each disorder has characteristic presentations, examination findings, radiographic characteristics, and treatment strategies.
Osteoarthritis is the most common degenerative process in the shoulder.8 Classic presentation includes progressive atraumatic pain, loss of motion, morning stiffness, and a concomitant loss of strength. Radiographic signs of glenohumeral osteoarthritis include osteophyte formation, loss of joint space, subchondral sclerosis, and osseous cyst formation (Figure 1, A). Posterior glenoid wear and posterior humeral head subluxation are common in later stages of the disease. Surgical treatment includes arthroscopic débridement, capsular release, surface replacement or hemiarthroplasty, and total shoulder arthroplasty (TSA) (reverse and anatomic).
 Figure 1 True AP radiographs demonstrating the classic findings of glenohumeral osteoarthritis (A), inflammatory arthritis (B), rotator cuff arthropathy (C), and osteonecrosis (D). |
Inflammatory arthritis, most commonly rheumatoid arthritis, is an inflammatory process characterized by a synovial disease that erodes the glenohumeral articulation.9 Painful motion, polyarticular disease, and loss of motion are common. The radiographic findings include periarticular erosions, subchondral cysts, osteopenia, and central glenoid wear, with medialization of the humeral head in advanced disease (Figure 1, B). The physician must be aware of the possible coexistence of joint infection because these patients are often on immunosuppressive medication and the clinical manifestations of rheumatoid arthritis are similar to those of infectious arthritis. Patients with rheumatoid arthritis and preserved joint space may benefit from arthroscopic synovectomy, whereas those with later-stage disease benefit from arthroplasty.
RCA describes a particular type of glenohumeral arthritis that develops in the setting of a massive chronic rotator cuff tear. Patients often have pseudoparalysis, with little active elevation or abduction of the shoulder. Radiographs demonstrate proximal migration of the humeral head and superior glenoid wear with loss of glenohumeral joint space (Figure 1, C). Acetabularization of the acromion can occur with end-stage RCA. Treatment for RCA was revolutionized by the development of the RSA.
Osteonecrosis is a less frequent disease of the shoulder, often found in younger patients with deep,
unexplained shoulder pain. It may be idiopathic or posttraumatic, or it may result from steroid usage, alcoholism, sickle cell disease, lupus, vascular compromise, and chemotherapy or irradiation.10 Disruption of the vascular supply to the humeral head leads to cartilage collapse and a loss of normal glenohumeral congruity, with subsequent pain, stiffness, and advanced glenohumeral arthritis (Figure 1, D). Treatment is guided by assessment of the etiology of the osteonecrosis and reversal of the offending cause, if possible, followed by radiographic assessment of subchondral collapse and glenoid involvement. Classification is based on a modified Ficat scheme. Core decompression is performed as an early intervention before significant subchondral collapse, whereas hemiarthroplasty may benefit patients with unipolar disease, and TSA is reserved for shoulders in which the glenoid has become involved.10
unexplained shoulder pain. It may be idiopathic or posttraumatic, or it may result from steroid usage, alcoholism, sickle cell disease, lupus, vascular compromise, and chemotherapy or irradiation.10 Disruption of the vascular supply to the humeral head leads to cartilage collapse and a loss of normal glenohumeral congruity, with subsequent pain, stiffness, and advanced glenohumeral arthritis (Figure 1, D). Treatment is guided by assessment of the etiology of the osteonecrosis and reversal of the offending cause, if possible, followed by radiographic assessment of subchondral collapse and glenoid involvement. Classification is based on a modified Ficat scheme. Core decompression is performed as an early intervention before significant subchondral collapse, whereas hemiarthroplasty may benefit patients with unipolar disease, and TSA is reserved for shoulders in which the glenoid has become involved.10
 Figure 2 True AP (A), AP (B), axillary (C), and scapular Y (D) views of the shoulder are the four views typically obtained when performing a radiographic evaluation of glenohumeral arthritis. |
Posttraumatic arthritis is a mixed group of disorders resulting from osseous, cartilaginous, or soft-tissue trauma. Tuberosity malunion, intra-articular fractures, and iatrogenic injury secondary to stabilization procedures (postcapsulorrhaphy) all can lead to glenohumeral arthrosis. Severe stiffness, particularly in external rotation, is noted in these conditions.
Presentation and Evaluation
The patient with significant glenohumeral arthritis usually presents with pain and loss of function. The history should include a description of the onset of the problem, any injuries, previous surgeries, attempts at nonsurgical management, and the nature and progression of functional difficulties. Systemic or polyarticular manifestations of sepsis, degenerative joint disease, or rheumatoid arthritis may provide helpful clues. A past history of steroid use or alcohol abuse may suggest osteonecrosis, whereas past injury, fractures, or stabilization surgery suggest posttraumatic or postcapsulorrhaphy arthropathy.
Physical examination of the shoulder begins with a thorough inspection for deformity, atrophy, scars, effusions, and swelling. Palpation of bony prominences (AC joint), bicipital groove, tuberosities, deltoid, and any areas of swelling is necessary. Evaluating range of motion in all planes (forward elevation, abduction, internal and external rotation), both passive and active, helps differentiate acquired stiffness versus weakness, which may indicate rotator cuff disease. Strength testing of the deltoid, rotator cuff, and scapular stabilizers includes testing of subscapularis function (lift-off, belly press, bear hug). Crepitus with motion is common in degenerative joint disease. Finally, a thorough neurovascular evaluation is performed, focusing on the axillary nerve (deltoid strength and lateral deltoid sensation).
Radiographic Imaging
Standard views include an AP view in the plane of the scapula (Grashey view), a standard AP view, scapular Y, and a true axillary view (Figure 2). These views will show humeral head and glenoid morphology, loss of glenohumeral joint space, and the relative positions of the humeral head and glenoid. The presence of osteophytes, deformity, subluxation, and erosion can be noted. A chronic massive rotator cuff tear likely exists in the case of proximal migration (Figure 1, C).
CT can be performed to quantify bone quality and geometry in complex arthritis cases. The Walch classification of glenoid morphology is based on wear patterns and version and is best assessed on CT scan (Figure 3). CT scans can also be used for three-dimensional preoperative planning and the creation of patient-specific implants.
Imaging of the rotator cuff by MRI, CT arthrogram, or ultrasonography is performed if it will affect patient management. However, rotator cuff assessment from patient history, physical examination, and radiographs is usually sufficient in the setting of glenohumeral arthrosis.
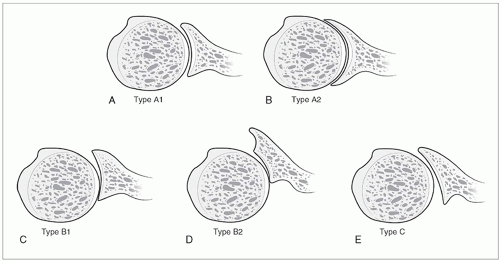 Figure 3 Illustrations of the glenohumeral joint demonstrating the Walch classification, based on version and wear pattern. A, Type A1: centered humeral head with minor concentric glenoid erosion. B, Type A2: centered humeral head with major concentric glenoid erosion. C, Type B1: posterior humeral subluxation with eccentric erosion. D, Type B2: posterior humeral subluxation with eccentric erosion with a biconcave glenoid. E, Type C: severe retroversion greater than 25°. (Reprinted from Sears BW, Johnston PS, Ramsey ML, Williams GR: Glenoid bone loss in primary total shoulder arthroplasty: Evaluation and management. J Am Acad Orthop Surg 2012;20[9]:604-613.) |
Nonsurgical Management
Nonsurgical management of glenohumeral arthritis is recommended initially and includes activity modification, anti-inflammatory medications, and physical therapy as first-line treatment strategies. Physical therapy can preserve motion and optimize function; however, attempts at therapy in the setting of substantial stiffness may worsen symptoms. Secondary treatment strategies include corticosteroid injections, local analgesics, and transdermal analgesics. Treatment options, such as acupuncture, electrical stimulation, ultrasound therapy, and oral supplements, may provide benefit but are not well studied. The use of disease-modifying antirheumatic drugs has decreased the incidence of shoulder arthroplasty in patients with rheumatoid/inflammatory arthritis.9
Joint-Preserving
Treatment Joint-preserving surgical treatment for shoulder arthritis is an option for mild disease, especially in younger adults in whom implant longevity is a concern or in situations in which the arthritis is localized to a focal area of chondral loss. Cartilage-preserving options include capsular release, glenohumeral débridement, and synovectomy. Cartilage restoration procedures include microfracture of focal chondral lesions, osteochondral autograft, autologous chondrocyte implantation, osteochondral allograft, and glenoid biologic resurfacing. A 2021 study showed good 10-year follow-up in young patients with glenohumeral osteoarthritis who underwent an arthroscopic comprehensive arthritis management procedure,11 which focuses on glenohumeral chondroplasty, synovectomy, loose body removal, humeral osteoplasty with excision of the inferior osteophyte, capsular release, subacromial and subcoracoid decompression, axillary nerve decompression, and biceps tenodesis. The survivorship rate at minimum 10-year follow-up was 63.2%.11
Hemiarthroplasty
Hemiarthroplasty was developed more than 50 years ago for the management of nonreconstructible proximal humeral fractures.12 The current indications for hemiarthroplasty include treatment of primary glenohumeral osteoarthritis in younger adults in whom the longevity of a glenoid component is of concern, arthritic conditions with inadequate glenoid bone stock, rotator cuff tear arthropathy, inflammatory arthropathy, and
osteonecrosis of the humeral head without secondary involvement of the glenoid.
osteonecrosis of the humeral head without secondary involvement of the glenoid.
Hemiarthroplasty must be indicated carefully as studies show improved survivorship with TSA as well as superior pain relief.13 One study of patients younger than 55 years with 10-year follow-up demonstrated 92% implant survival with TSA compared with 72% for hemiarthroplasty.14 Clinical success and survivorship of hemiarthroplasty are likely affected by patient-specific factors including glenoid morphology.
Hemiarthroplasty with concentric reaming of the glenoid, known as ream and run, is also an option, but studies demonstrate that men older than 60 years have better results than younger adults, and pain relief is delayed up to 1.5 years postoperatively.15 Hemiarthroplasty with biologic glenoid resurfacing has shown favorable short-term results but up to 30% revision rates.16
Related posts:
 Orthopaedic Patient Safety: Core Competencies and Communication Skills
New Technology in Orthopaedic Surgery: Robotics, Artificial Intelligence, and Machine Learning
Applications of Three-Dimensional Technologies in Orthopaedic Surgery
Shoulder Anatomy, Biomechanics, Clinical Evaluation, and Imaging
Ligament Injuries of the Wrist
Articular Cartilage of the Knee: Defects, Degeneration, and Preservation
Orthopaedic Patient Safety: Core Competencies and Communication Skills
New Technology in Orthopaedic Surgery: Robotics, Artificial Intelligence, and Machine Learning
Applications of Three-Dimensional Technologies in Orthopaedic Surgery
Shoulder Anatomy, Biomechanics, Clinical Evaluation, and Imaging
Ligament Injuries of the Wrist
Articular Cartilage of the Knee: Defects, Degeneration, and Preservation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


