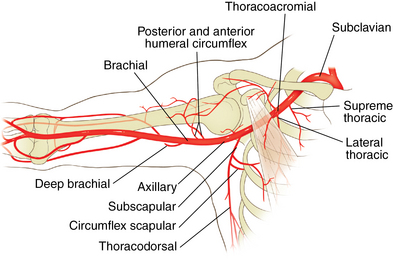
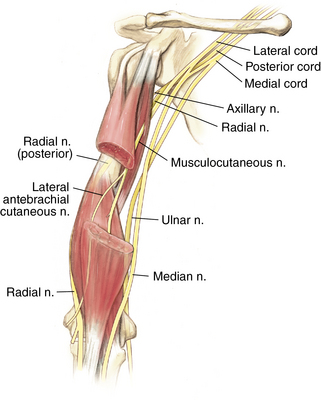
2 Shoulder and humerus Figure 2-8. Major branches of the brachial plexus in the upper arm. (From Miller MD, Chhabra AB, Hurwitz SR, et al, editors: Orthopaedic surgical approaches, Philadelphia, 2008, Saunders, p 17.) Inspect for deformity or muscle atrophy. Palpate the specific structures to evaluate for deformity or tenderness: Normal range of motion (ROM): Table 2-1 Table 2-1. Normal Shoulder Range of Motion Table 2-2. • Pain medication refill, if necessary • Discontinuation of sling as tolerated • Review of work status, light duty desk work generally for 6 weeks • These patients are significantly weak on examination and may demonstrate a drop arm sign. • Diagnosis can be made by plain radiographs when proximal migration of the humeral head relative to the glenoid is seen (Fig. 2-14). • Physical therapy orders given to focus on passive ROM of the shoulder only • Pain medication refill, if necessary • Continued use of sling removing only for pendulum exercises and elbow motion • Review of work status; light duty desk work begun as tolerated by patient, with no use of surgical arm • Evaluation of wound healing, ROM, and strength • New physical therapy orders to begin active-assisted ROM, active motion, and gentle early rotator cuff strengthening exercises • Light duty work continued for a minimum of 6 additional weeks
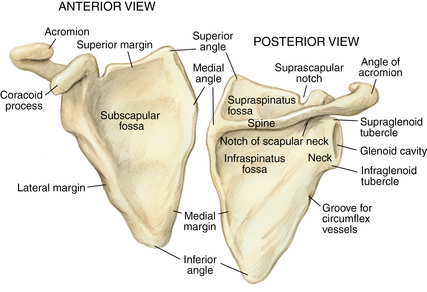
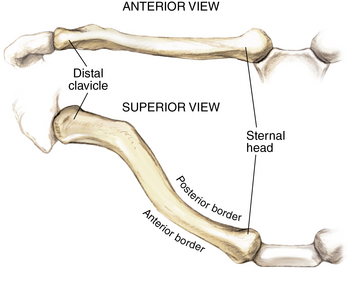
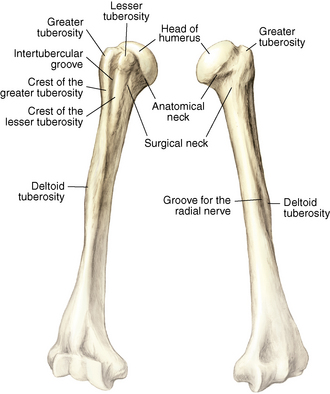
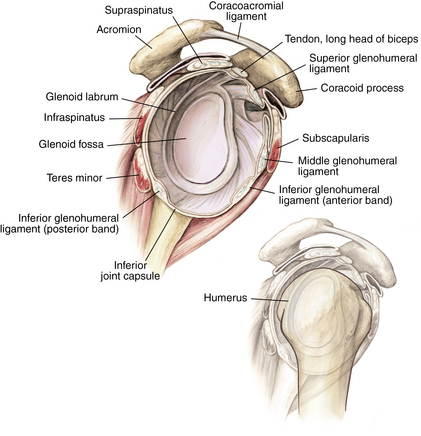
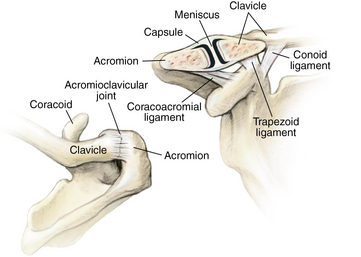
Anatomy of joint
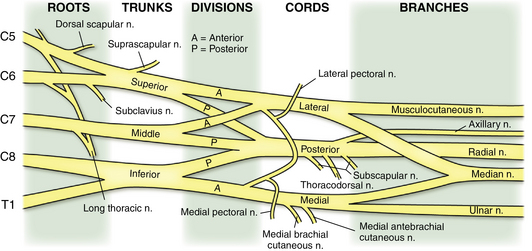
Nerves and arteries: Figures 2-7 through 2-9
Physical examination
Forward Flexion
180 degrees
Abduction
180 degrees
External Rotation
90 degrees
Internal Rotation
90 degrees
Special tests
Belly press test
Differential diagnosis: Table 2-2
Anterior shoulder pain
Shoulder impingement
Biceps tendinitis
Arthritis
Rotator cuff tear
Instability
Labral tear
Posterior shoulder pain
Periscapular muscle pain
Posterior instability
Cervical radiculopathy
Posterior labral tear
Subscapular bursitis
Scapula fracture
Superior shoulder pain
Acromioclavicular joint osteolysis
Acromioclavicular joint arthritis
Clavicle fracture
Shoulder (AC) separation
Superior labral tear
Arm pain
Humerus fracture
Rotator cuff tear
Shoulder impingement
Cervical radiculopathy
Shoulder impingement
Initial treatment
 Shoulder impingement is part of the spectrum of rotator cuff injury. Generally, in the early stages this involves inflammation (bursitis and rotator cuff tendinitis) without actual tearing of the tendon. Partial tears can develop over time and can progress to a full-thickness tear. If symptoms do not improve with early treatment, call the office because a magnetic resonance imaging (MRI) scan may be necessary to evaluate for a rotator cuff tear.
Shoulder impingement is part of the spectrum of rotator cuff injury. Generally, in the early stages this involves inflammation (bursitis and rotator cuff tendinitis) without actual tearing of the tendon. Partial tears can develop over time and can progress to a full-thickness tear. If symptoms do not improve with early treatment, call the office because a magnetic resonance imaging (MRI) scan may be necessary to evaluate for a rotator cuff tear.
Treatment options
 Nonoperative management is indicated if the patient has pain without evidence of a full-thickness rotator cuff tear (night pain, weakness on examination, history of recent shoulder dislocation in patient over the age of 40 years).
Nonoperative management is indicated if the patient has pain without evidence of a full-thickness rotator cuff tear (night pain, weakness on examination, history of recent shoulder dislocation in patient over the age of 40 years).
 Treatment generally begins with the addition of NSAIDs and/or subacromial steroid injection.
Treatment generally begins with the addition of NSAIDs and/or subacromial steroid injection.
 Prognosis for shoulder impingement is good with these nonsurgical treatment options.
Prognosis for shoulder impingement is good with these nonsurgical treatment options.
 Generally the patient should be reevaluated in 6 weeks to check ROM and strength.
Generally the patient should be reevaluated in 6 weeks to check ROM and strength.
Operative management: Subacromial decompression
Codes
Informed consent and counseling
 Routine surgical risks should be discussed with the patient (infection, bleeding, bruising, surgical pain, continued symptoms, and anesthesia complications).
Routine surgical risks should be discussed with the patient (infection, bleeding, bruising, surgical pain, continued symptoms, and anesthesia complications).
 Physical therapy is generally expected after surgery for approximately 6 weeks.
Physical therapy is generally expected after surgery for approximately 6 weeks.
 Informed consent should include the possibility of rotator cuff repair if an unexpected tear is discovered at the time of surgery because this could lead to a longer recovery time (6 weeks in a sling and an average of 12 weeks of physical therapy).
Informed consent should include the possibility of rotator cuff repair if an unexpected tear is discovered at the time of surgery because this could lead to a longer recovery time (6 weeks in a sling and an average of 12 weeks of physical therapy).
Surgical procedures
 The posterior portal is first created as the primary viewing portal for the arthroscope, followed by the anterior portal (working portal) for instruments.
The posterior portal is first created as the primary viewing portal for the arthroscope, followed by the anterior portal (working portal) for instruments.
 A lateral portal can be made to pass instruments for the acromioplasty.
A lateral portal can be made to pass instruments for the acromioplasty.
 Adequate bony resection should be confirmed before removing the arthroscope and closing the portals.
Adequate bony resection should be confirmed before removing the arthroscope and closing the portals.
Estimated postoperative course
 Initial postoperative visit (7 to 14 days)
Initial postoperative visit (7 to 14 days)
 12-week postoperative visit (optional)
12-week postoperative visit (optional)
Rotator cuff tears
 Pain is located in the anterior and lateral shoulder.
Pain is located in the anterior and lateral shoulder.
 Pain frequently radiates to the deltoid area, but not usually below elbow.
Pain frequently radiates to the deltoid area, but not usually below elbow.
 Tears are generally atraumatic, with progression of pain and weakness over time.
Tears are generally atraumatic, with progression of pain and weakness over time.
 They may be related to an acute trauma (e.g., fall on the outstretched hand).
They may be related to an acute trauma (e.g., fall on the outstretched hand).
 Waking at night is one of the frequently described symptoms.
Waking at night is one of the frequently described symptoms.
 The patient may or may not complain of weakness in that arm.
The patient may or may not complain of weakness in that arm.
Physical examination
 Active ROM may be limited, but passive ROM is generally full.
Active ROM may be limited, but passive ROM is generally full.
 Hawkins and Neer impingement signs may or may not be present.
Hawkins and Neer impingement signs may or may not be present.
 The supraspinatus stress test (weak with resisted abduction) is positive.
The supraspinatus stress test (weak with resisted abduction) is positive.
 Weakness with resisted external rotation indicates involvement of the infraspinatus.
Weakness with resisted external rotation indicates involvement of the infraspinatus.
 A positive lift-off or belly press sign indicates involvement of the subscapularis.
A positive lift-off or belly press sign indicates involvement of the subscapularis.
 A positive O’Brien sign indicates involvement of the biceps tendon.
A positive O’Brien sign indicates involvement of the biceps tendon.
Imaging
Classification system
 Rotator cuff tears are typically described by the number of tendons involved, the size of the tear, the amount of tendon retraction, and the degree of fatty atrophy of the rotator cuff muscles.
Rotator cuff tears are typically described by the number of tendons involved, the size of the tear, the amount of tendon retraction, and the degree of fatty atrophy of the rotator cuff muscles.
Initial treatment
 Initial treatment is determined by the size of the rotator cuff tear.
Initial treatment is determined by the size of the rotator cuff tear.
 High-grade partial rotator cuff tears (involving >50% of the total tendon area) may be treated conservatively but may require surgical repair. This decision is determined by the degree of the patient’s pain and dysfunction and the severity of the tear (for a 60% tear, an attempt at conservative treatment is more likely, whereas a 90% tear may suggest the need for earlier operative intervention).
High-grade partial rotator cuff tears (involving >50% of the total tendon area) may be treated conservatively but may require surgical repair. This decision is determined by the degree of the patient’s pain and dysfunction and the severity of the tear (for a 60% tear, an attempt at conservative treatment is more likely, whereas a 90% tear may suggest the need for earlier operative intervention).
 Complete rotator cuff repairs should be treated with surgery in most cases.
Complete rotator cuff repairs should be treated with surgery in most cases.
Patient education
Treatment options
Operative management: Rotator cuff repair
Informed consent and counseling
Surgical procedures
 For arthroscopic repair, the posterior portal is first created as the primary viewing portal for the arthroscope, followed by the anterior portal (working portal) for instruments.
For arthroscopic repair, the posterior portal is first created as the primary viewing portal for the arthroscope, followed by the anterior portal (working portal) for instruments.
 Acromioplasty is typically performed as described earlier.
Acromioplasty is typically performed as described earlier.
 Partial-thickness tears of less than 50% can be débrided with the shaver rather than repaired.
Partial-thickness tears of less than 50% can be débrided with the shaver rather than repaired.
 Full-thickness tears and high-grade partial tears must be mobilized and repaired.
Full-thickness tears and high-grade partial tears must be mobilized and repaired.
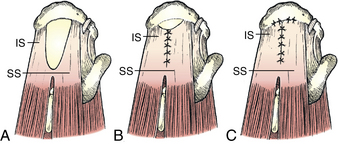
 Margin convergence may be necessary before direct repair of tendon back to bone in the case of L-shaped or U-shaped tears (Fig. 2-15).
Margin convergence may be necessary before direct repair of tendon back to bone in the case of L-shaped or U-shaped tears (Fig. 2-15).
Estimated postoperative course
 Initial postoperative visit (7 to 14 days)
Initial postoperative visit (7 to 14 days)
Shoulder and humerus