Chapter 9 Shoulder and Elbow Reduction
Clavicle fracture
Pearls
1. Clavicle fractures with more than 1.5 cm of overlap result in long-term disability and should be treated with an open reduction and internal fixation.
2. Fractures that tent the skin can erode through the skin and are unlikely to heal without open reduction and internal fixation.
3. There is no difference in outcome between a figure-of-8 splint and a sling for closed management of clavicle fractures.
Acromioclavicular separation


Pearls
1. AC separations with severe displacement or soft tissue interposition (grades 4 to 6) should be reduced surgically on an elective basis.
Glenohumeral dislocation
Overview
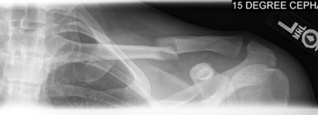
3. An axillary or modified axillary view is an essential part of the radiographic series (Figure 9-4)!

Precautions
1. Confirm that no fracture is present on diagnostic films before attempting a reduction. Standard reduction maneuvers can result in a displaced four-part fracture that requires surgical fixation/prosthetic replacement.
2. Confirm that the humeral head is not impacted onto the glenoid (known as a Hill-Sachs lesion) before attempting a reduction (see Figure 9-4). Standard reduction maneuvers can result in a head-splitting fracture.
3. When applying traction, make sure that the force is applied over a broad area; otherwise, a forearm fracture can result.
4. Be aware that some persons may voluntarily initiate a glenohumeral dislocation in an effort to gain access to drugs.
5. Reducing dislocations in persons who present more than a few days after the injury may not be possible, and attempting to do so could result in a fracture; it is preferable not to attempt a reduction and to take the patient to the operating room if simple traction does not succeed in reducing the dislocation.
Pearls
1. Be patient; the stability of the shoulder is provided largely by a set of small but powerful muscles that must be overcome with gentle sustained traction before a reduction is possible.
3. For posterior dislocations, stretching the rotator cuff muscles by maximal internal rotation of the shoulder may be necessary.
5. External rotation is a better position for immobilization of both anterior and posterior dislocations after reduction, although a gunslinger brace may not be available immediately.
Anterior glenohumeral dislocation
Detailed Technique
3. Prepare traction setup:
b. Slide a rolled bed sheet around the patient’s trunk under the ipsilateral shoulder and tie it over the contralateral upper corner of the stretcher for countertraction (Figures 9-5 and 9-6).
4. Apply traction:
a. Position yourself along the ipsilateral side of the stretcher so that the shoulder is slightly abducted.
8. Place the arm in a sling (see Chapter 13) in internal rotation or in a gunslinger brace in external rotation.















