Shilla
Richard E. McCarthy
The Shilla procedure is based upon a concept that once the apex of the spinal deformity is corrected, the normal part of the spine can be guided to grow into a normal coronal and sagittal alignment with spinal growth as the engine for change. The restoration of normal alignment in all planes at the apex is key to restoring a horizontal position to the discs above and below the apex. This places the apophyses in a position to grow and increase height of the spine.
Guided growth can be applied to any degree of curvature, but our experience has been solely confined to patients with severe (greater than 50 degrees) spinal deformities. At the time of this writing, 76 patients have been treated with the Shilla procedure at our home institution (Arkansas Children’s Hospital) and constitute the basis for these conclusions.
Patients are selected to undergo this procedure based upon the curve size (greater than 50 degrees), the amount of growth remaining, the ability of the child to undergo 4 to 5 hours of surgery, the ability of the child to benefit from the surgery, and the need to prevent thoracic insufficiency. All diagnoses of early-onset scoliosis have been treated with this method. Preoperative planning is of key importance for each patient in order to maximize correction and the coordination of the surgical team. Accordingly, a preoperative blueprint has been found to be very helpful in summarizing the conclusions drawn from the assessment of the flexibility films as well as the plans for anticipated implants and corrective maneuvers.
The ultimate goal is to realign the apical segments (those least derotated on the flexibility films) into a neutral alignment in all planes—coronal, sagittal, and axial. For most cases, this has comprised three or four vertebral segments, occasionally only two vertebrae (i.e., very flexible curves). Firm bilateral fixed head pedicle screw fixation will permit maximum force on the vertebra to derotate and translate during correction maneuvers and overcome growth forces over time to prevent crankshaft (1, 2). It has been the editor’s (dls) experience that crankshaft develops in a substantial portion of children who have a Shilla procedure at a young age. Ponte osteotomies between the apical segments will improve flexibility and correction. The apical segments are the only levels approached subperiosteally and then decorticated for fusion and firm fixation to the rods. Allograft or autograft has been used to accomplish fusion.
The blueprint is a working document that encompasses the preoperative plans for site (level) and type of screw but is a “working document” modified according to intraoperative findings.
The screws should fill the pedicle and be placed deeply into the vertebra to supply maximum fixation with fixed head (or monoaxial) screws at the apex and polyaxial screws used as growing screws. The Shilla cap fixes to the screw instead of the rod to allow sliding of the rod with growth. A cross-link links the two rods adjacent to the apex to strengthen the construct and overcome the tendency for rod rotation. An expandable cross-link has been used in children less than 5 years of age to prevent the theoretical problem of spinal canal stenosis (Fig. 47-1).
SURGICAL PROCEDURE
The procedure is performed through a single incision the length of the construct, directed through the subcutaneous layers without incision of fascia or spinous processes. With fluoroscopy and sterile needles, the spinous processes of the vertebral levels are identified and written along the side of the wound on the sterile drape. A subperiosteal dissection of the apical segments only is done
with cleaning of soft-tissue attachments to enhance fusion of these segments. The fascia is incised linearly one centimeter on each side of the spinous processes cephalad and caudal to the apex. It is through the muscle layer that the growing screws will be placed fluoroscopically. The apical screws are placed after the Ponte osteotomies, checking the screw placement in AP and lateral views with the C-arm (Fig. 47-2). Using Jamshidi needles with the C-arm in the AP plane, cannulation wires are placed into the center at the pedicles of the sites planned for the growing screws. The pedicles are tapped with a tapered cannulated tap, half the depth of the pedicle. A cannulated, polyaxial screw is placed at least three quarter’s across the width of the vertebra, the largest diameter screw permissible to maximize fixation. A PediGuard Jamshidi has been helpful to minimize fluoroscopic irradiation and aid in accurate screw placement. Lumbar growing screws have been placed bilaterally at the same levels, leaving an uninstrumented level between screws to enhance sliding of the rods. The cephalad-growing screws are most commonly placed in an alternating fashion, spread through the upper thoracic spine. The screws are checked fluoroscopically as well as with direct screw stimulation to insure proper placement (Fig. 47-3).
with cleaning of soft-tissue attachments to enhance fusion of these segments. The fascia is incised linearly one centimeter on each side of the spinous processes cephalad and caudal to the apex. It is through the muscle layer that the growing screws will be placed fluoroscopically. The apical screws are placed after the Ponte osteotomies, checking the screw placement in AP and lateral views with the C-arm (Fig. 47-2). Using Jamshidi needles with the C-arm in the AP plane, cannulation wires are placed into the center at the pedicles of the sites planned for the growing screws. The pedicles are tapped with a tapered cannulated tap, half the depth of the pedicle. A cannulated, polyaxial screw is placed at least three quarter’s across the width of the vertebra, the largest diameter screw permissible to maximize fixation. A PediGuard Jamshidi has been helpful to minimize fluoroscopic irradiation and aid in accurate screw placement. Lumbar growing screws have been placed bilaterally at the same levels, leaving an uninstrumented level between screws to enhance sliding of the rods. The cephalad-growing screws are most commonly placed in an alternating fashion, spread through the upper thoracic spine. The screws are checked fluoroscopically as well as with direct screw stimulation to insure proper placement (Fig. 47-3).
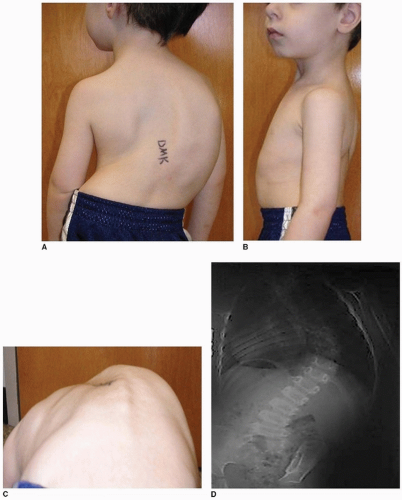 FIGURE 47-1 A-C. 3 + 1-year-old with infantile idiopathic scoliosis. D, E.
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|
