Scapular Winging Caused by Serratus Anterior Dysfunction: Recognition and Treatment
Philippe Clavert
Jon J. P. Warner
P. Clavert and J. J. P. Warner: The Harvard Shoulder Service, Department of Orthopaedic Surgery, Massachusetts General Hospital, Boston, Massachusetts.
INTRODUCTION
Scapular winging may be associated with several neurologic conditions including spinal accessory nerve palsy and fascioscapulohumeral muscular dystrophy; however, it is most commonly associated with isolated paralysis of the long thoracic nerve. Whether of idiopathic or traumatic cause, scapular winging may vary from complete paralysis to paresis, and most cases resolve within 18 months.56 For this reason, all patients must be treated conservatively when the diagnosis is made, and consideration for surgery is only in the most chronic cases. Diagnosis and surgical management of refractory scapular winging caused by serratus anterior dysfunction will be presented in this chapter.
HISTORICAL PERSPECTIVE
Winslow first reported the clinical presentation of scapular winging in 1777.66 Velpeau60 in 1837 was the first to isolate the pathoanatomy of the winging and described a case of an isolated serratus anterior palsy. Subsequently, other authors have reported their experiences in the literature.10,11,19,22,44,48,50,52,58,63,65,68
The first surgical treatment was described by Tubby in 1904.57 He transferred the sternal portion of the pectoralis major to the different digitations of the serratus anterior. But as the serratus was denervated, the graft progressively stretched out and a recurrence of the scapular winging occurred. Others suggested a fascial sling suspension operation as surgical treatment.4,31,64 As with the prior techniques, the recurrence of scapular winging was high because the graft stretched out64; thus, scapulothoracic fusion was proposed and developed.13,20 Scapulothoracic fusion, however, resulted in more motion loss, so some surgeons developed a method of dynamic scapular stabilization by
transferring muscles. Numerous tendon transfers were thus developed, including the pectoralis minor,10,50,58 pectoralis major or split pectoralis major,11,44,48,52,63,65 teres major,19,68 and rhomboideus muscle.22 Currently, the two techniques routinely used to treat winging caused by long thoracic nerve palsy are the split pectoralis major tendon transfer and scapulothoracic fusion.
transferring muscles. Numerous tendon transfers were thus developed, including the pectoralis minor,10,50,58 pectoralis major or split pectoralis major,11,44,48,52,63,65 teres major,19,68 and rhomboideus muscle.22 Currently, the two techniques routinely used to treat winging caused by long thoracic nerve palsy are the split pectoralis major tendon transfer and scapulothoracic fusion.
Marmor and Bechtol in 196338 first described transfer of the sternal head of the pectoralis tendon. Their original technique was with a fascia lata graft extension. This technique requires a large incision over the shoulder and hemithorax as well as a large incision on the lateral thigh. Post48 and others11,40,44,48 subsequently refined this technique and reported good success with it. Unfortunately, some patients experienced pain at the donor site of fascia lata graft harvested from the thigh. This morbidity was caused by muscle herniation and development of seromas. Subsequently, others have described smaller incisions on the shoulder and thorax as well as the use of semitendinosus and gracilis tendons, which may be harvested through a smaller incision with less morbidity.41,54,63
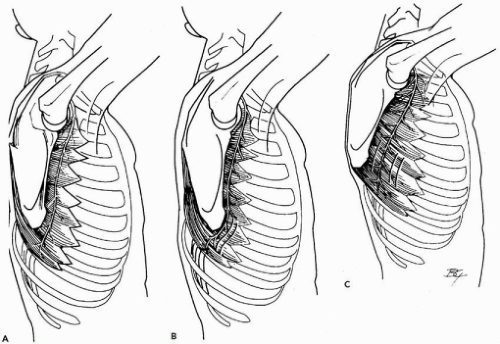 Figure 31-1 (A-C) Insertions of the serratus anterior on the lateral aspect of the chest wall and of the long thoracic nerve course. Mechanism of injury of the long thoracic nerve stretched while the arm is protracted. (Reprinted with permission from: Kuhn JE, Hawkins RJ. Evaluation and treatment of scapular disorders. In: Warner JJP, Iannotti JP, Gerber C, eds. Complex and revision problems in shoulder surgery. 1st edition. Philadelphia, PA, Lippincott-Raven, 1997.) |
SCAPULAR WINGING AND SERRATUS ANTERIOR DYSFUNCTION
Anatomy
The serratus anterior muscle is a large muscle that expands over the lateral aspect of the thorax. Digitations arise from the upper first nine ribs, pass between the scapula and the ribs, and attach to the medial border of the scapula (Fig. 31-1). The long thoracic nerve is the sole innervator of the serratus anterior and is purely a motor nerve. It originates
from the ventral rami of the C5 and C6 cervical roots. Some fibers coming from C7 may also participate in the innervation of the serratus anterior. The C5 and C6 roots pass through the scalenus medius muscle and merge before they receive a branch from the seventh cervical root. The long thoracic nerve then courses beneath the clavicle, over the first rib, and beneath the brachial plexus. Once on the chest wall, the long thoracic nerve courses to the serratus anterior muscle slips and ends at the inferior angle of the scapula (Fig. 31-1). This superficial and winding course and its length make this nerve at risk for low-energy compression injuries and stretch injuries.1,23,25
from the ventral rami of the C5 and C6 cervical roots. Some fibers coming from C7 may also participate in the innervation of the serratus anterior. The C5 and C6 roots pass through the scalenus medius muscle and merge before they receive a branch from the seventh cervical root. The long thoracic nerve then courses beneath the clavicle, over the first rib, and beneath the brachial plexus. Once on the chest wall, the long thoracic nerve courses to the serratus anterior muscle slips and ends at the inferior angle of the scapula (Fig. 31-1). This superficial and winding course and its length make this nerve at risk for low-energy compression injuries and stretch injuries.1,23,25
 Figure 31-2 (A,B) Clinical presentation of a patient presenting a scapular winging. |
Biomechanics
The serratus anterior muscle protracts and rotates the scapula around the thorax. Thus, the scapula is pulled forward during elevation of the arm. This motion is essential to permit full overhead elevation as it tilts the glenoid forward and upward allowing the humeral head to rotate on a fixed joint platform. An injury to the long thoracic nerve results in paradoxic movement of the scapula away from the chest so that the inferior angle of the scapula rotates toward the midline and the medial border of the scapula becomes prominent. This is observed as winging (Fig. 31-2). The biomechanical consequences of such paradoxic motion are to reduce the arc of motion available to the glenohumeral joint so the humerus cannot move upward because of loss of mechanical advantage of the deltoid and rotator cuff. Furthermore, the humerus will contact the coracoacromial arch, which can cause non-outlet impingement. This may be why a rotator cuff problem is misdiagnosed in some of these patients (Fig. 31-3).
Cause
In most cases, injury to the long thoracic nerve is neurapraxic because of stretching or compression (Fig. 31-1). This explains why most cases improve with conservative treatment. Both traumatic and nontraumatic events may
cause this problem. Described causes include the rare condition of nerve entrapment into the scalenus muscle or by the first rib,17,18,30 nontraumatic injuries to the long thoracic nerve from compression of the nerve while the arm is abducted,59 viral illnesses,15,49 immunization,5 Parsonage-Turner syndrome,42 and isolated long thoracic neuritis.47,49 Iatrogenic lesions of the long thoracic nerve have also been reported, mainly after radical mastectomy, first rib resection for outlet syndrome, and transaxillary sympathectomy.16,30,59
cause this problem. Described causes include the rare condition of nerve entrapment into the scalenus muscle or by the first rib,17,18,30 nontraumatic injuries to the long thoracic nerve from compression of the nerve while the arm is abducted,59 viral illnesses,15,49 immunization,5 Parsonage-Turner syndrome,42 and isolated long thoracic neuritis.47,49 Iatrogenic lesions of the long thoracic nerve have also been reported, mainly after radical mastectomy, first rib resection for outlet syndrome, and transaxillary sympathectomy.16,30,59
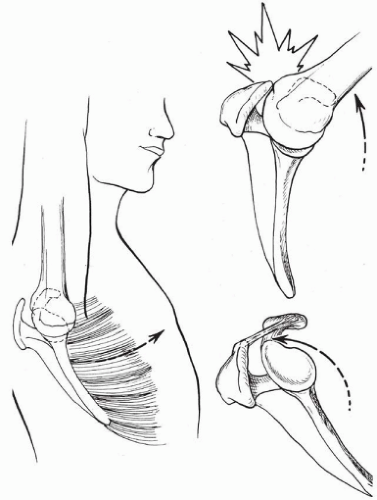 Figure 31-3 Serratus anterior dysfunction and its role in subacromial impingement and rotator cuff disease. (Reprinted with permission from: Kuhn JE, Hawkins RJ. Evaluation and treatment of scapular disorders. In: Warner JJP, Iannotti JP, Gerber C, eds. Complex and revision problems in shoulder surgery. 1st edition. Philadelphia, PA, Lippincott-Raven, 1997.) |
Traumatic injuries to the long thoracic nerve occur mainly after sudden traction to the upper limb during a fall or collision, at work, or during sports or daily living activities.17,37,59,63 The nerve is stretched from its points where it is tethered: first rib, inferior border of the scapula, and first two or last branches of the nerve.2,17,23,29,67 Finally, in some patients, no cause for serratus anterior palsy can be identified.44,61,63 No matter what the cause, chronic winging may cause significant shoulder pain and disability.30
APPROACH TO DIAGNOSIS
Patient Presentation
Patients may often simply present with pain and/or weakness as the chief complaint, but they may not notice winging. This is why delay in diagnosis is not particularly rare. Indeed, many patients present whose treatments for a variety of other diagnoses have failed, including impingement, instability, and acromioclavicular disease.45,47,63
Pain is typically described as posterior around the scapula, and this seems to be caused by compensation of the remaining axioscapular muscles (rhomboids, trapezius). As noted previously, there may be impingement-type symptoms that occur because of a non-outlet impingement mechanism (Fig. 31-3).
Sometimes the patient or a family member may notice the winging when trying to elevate the arm, and in most cases there is difficulty with activities of daily living. More severe pain may indicate an acute plexus neuritis.49
Clinical Findings
All patients should be examined with their shirts off and the shoulders viewed from anterior and posterior during elevation of the arms. Muscle atrophy is usually not noticed in these patients, although subtle malpositioning of the scapula may be apparent. Some patients may have a scapula that actually sits in a slightly winged position. If the scapula is ptotic and sits lower than the contralateral side, and if the patient is unable to symmetrically shrug both shoulders, trapezius palsy should be suspected (Fig. 31-4).63
While the back of the patient is being viewed, he or she is asked to flex both shoulders, and scapular rhythm and stabilization are observed. Winging may be obvious, although in husky individuals it may still appear to be subtle. Total flexion will be limited in most patients (Fig. 31-2). It may be helpful for the examiner to keep the inferior angle of the scapula between his or her first two fingers to assess the scapulothoracic rhythm and winging. Several maneuvers will enhance winging by placing the serratus anterior at a mechanical disadvantage. The first maneuver is to have the patient place his or her hands on the wall and perform a push-up away from the wall.55 Winging may be apparent with this motion. The second maneuver is to have the patient resist flexion with the shoulders at 90 degrees, because this will overpower the stronger lower portion of the serratus anterior muscle.63
Related posts:
 Traumatic Anterior Instability: Arthroscopic Solutions
Traumatic Anterior Instability: Arthroscopic Solutions
 Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
 Acromioclavicular Joint: Difficult Problems and Revision Surgery
Acromioclavicular Joint: Difficult Problems and Revision Surgery
 Rotator Cuff Arthropathy: The Unconstrained Arthroplasty
Rotator Cuff Arthropathy: The Unconstrained Arthroplasty
 Scapular Winging: Trapezius Dysfunction
Scapular Winging: Trapezius Dysfunction
 Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


