Scapular Winging: Trapezius Dysfunction
Julie Y. Bishop
Evan L. Flatow
J. Y. Bishop: Clinical Shoulder Fellow, Department of Orthopaedic Surgery, Mount Sinai Medical Center, New York, New York.
E. L. Flatow: Lasker Professor of Orthopaedic Surgery, Chief of Shoulder Surgery, Department of Orthopaedic Surgery, Mount Sinai Medical Center, New York, New York.
INTRODUCTION
The trapezius is the major suspensory muscle of the shoulder girdle contributing to scapulothoracic rhythm by elevating, rotating, and retracting the scapula. Injury to the spinal accessory (eleventh cranial) nerve can cause significant dysfunction of this muscle.19,38 Paralysis of the trapezius results in drooping of the entire shoulder girdle, winging and lateral displacement of the scapula, and weakness in forward elevation and abduction.4,9,22 This constellation of symptoms can lead to considerable pain, deformity, and loss of function.
CAUSE
The spinal accessory nerve is located in the subcutaneous tissue on the floor of the posterior cervical triangle. This superficial location makes it very vulnerable to iatrogenic injury, which is the leading cause of trapezius paralysis.24,45 In the 1930s, removal of tuberculous lymph nodes in the neck was a common procedure, in which up to 10% of cases were complicated by injury to the spinal accessory nerve.16,30,47,48 As the incidence of trapezius nerve palsies peaked in the 1950s, concern mounted as it became clear that the morbidity associated with surgery in the posterior cervical triangle was very significant and problematic. Newer techniques and modified procedures have been proposed to protect the nerve during head and neck surgery.2,6 Nevertheless, sacrificing the nerve is sometimes necessary in radical neck dissections for cancer. The spinal accessory nerve may also be injured in anterior neck surgery, such as carotid endarterectomies.39,40 It has also been used as a graft for facial nerve paralysis and brachial plexus lesions; however, other graft sources are currently preferentially used.1,32
Trapezius palsy and dysfunction can also occur after blunt trauma and traction injuries to the spinal accessory nerve. Direct trauma can occur during contact sports, resulting, for example, from a blow from a hockey or lacrosse stick. Traction injuries can occur from motor vehicle accidents, falls from a height, sternoclavicular or acromioclavicular dislocations, or even extended use of an arm sling. Although rare, spontaneous onset of spinal accessory nerve paralysis has been reported.13,25
ANATOMY AND BIOMECHANICS
Periscapular Musculature
The scapula floats on the chest wall on a bed of muscles. The trapezius, levator scapulae, rhomboids, and serratus anterior muscles make up the scapular rotator group whose functions include passive support of the shoulder, active elevation of the shoulder, and rotation of the scapula (Fig. 32-1A). Codman6 was the first to elaborate on the importance of the fine balance among the muscles of the shoulder girdle that support the scapula; he described the concept of scapulohumeral rhythm. Inman et al.22 later showed the contribution of the trapezius to the
balance of the scapular rotary-force couples. Scapular and humeral motion occur simultaneously during upper extremity movement, and the trapezius is one of the primary movers of the scapula.22 The trapezius is the largest and most superficial of the scapulothoracic muscles. Its primary origin is the spinous processes of C7 down to T12. Above C7, the upper portion originates from the ligamentum nuchae up to the external occipital protuberance.23 It is divided into three distinct anatomic components: upper, middle, and lower (Fig. 32-1B). The upper portion inserts on the posterior border of the lateral third of the clavicle and rotates and elevates the scapula. The intermediate portion inserts on the medial acromion and along the superior lip of the spine of the scapula and is responsible for stability and adduction of the scapula. The inferior portion inserts on the base of the spine of the scapula and rotates the scapula downward and depresses it. All three portions of the trapezius work synchronously, and, overall, they work together to elevate, retract, and rotate the scapula. The trapezius is the only muscle to insert on the lateral tip of the scapula; thus, one of its most important functions is to elevate the lateral tip of the scapula and, by extension, the rest of the upper extremity. Therefore, trapezius paralysis will lead to drooping of the entire extremity, because the inferior border of the scapula rotates laterally.2,27 The levator scapulae, rhomboids, and serratus anterior are able to compensate to a certain extent, allowing some elevation above the horizontal plane. However, the inferior and laterally positioned scapula places the rhomboids and, to a lesser extent, the levator scapulae at a distinct biomechanical disadvantage, and maximal force generation is compromised.2,15
balance of the scapular rotary-force couples. Scapular and humeral motion occur simultaneously during upper extremity movement, and the trapezius is one of the primary movers of the scapula.22 The trapezius is the largest and most superficial of the scapulothoracic muscles. Its primary origin is the spinous processes of C7 down to T12. Above C7, the upper portion originates from the ligamentum nuchae up to the external occipital protuberance.23 It is divided into three distinct anatomic components: upper, middle, and lower (Fig. 32-1B). The upper portion inserts on the posterior border of the lateral third of the clavicle and rotates and elevates the scapula. The intermediate portion inserts on the medial acromion and along the superior lip of the spine of the scapula and is responsible for stability and adduction of the scapula. The inferior portion inserts on the base of the spine of the scapula and rotates the scapula downward and depresses it. All three portions of the trapezius work synchronously, and, overall, they work together to elevate, retract, and rotate the scapula. The trapezius is the only muscle to insert on the lateral tip of the scapula; thus, one of its most important functions is to elevate the lateral tip of the scapula and, by extension, the rest of the upper extremity. Therefore, trapezius paralysis will lead to drooping of the entire extremity, because the inferior border of the scapula rotates laterally.2,27 The levator scapulae, rhomboids, and serratus anterior are able to compensate to a certain extent, allowing some elevation above the horizontal plane. However, the inferior and laterally positioned scapula places the rhomboids and, to a lesser extent, the levator scapulae at a distinct biomechanical disadvantage, and maximal force generation is compromised.2,15
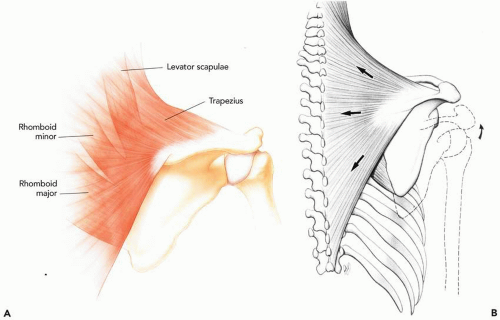 Figure 32-1 (A) Posterior view of the scapula with the trapezius, rhomboids, and levator scapulae muscles. (B) Normal function of the trapezius: the upper portion rotates and elevates the scapula, the middle portion stabilizes and adducts it, and the lower portion rotates the scapula downward and depresses it. |
Spinal Accessory Nerve
The spinal accessory nerve, cranial nerve XI, is the sole motor innervation to the trapezius muscle. It also supplies the sternocleidomastoid. It may be joined by proprioceptive branches from the second, third, or fourth cervical nerves.8,19 After supplying the sternocleidomastoid muscle, the spinal accessory nerve descends obliquely in the posterior triangle of the neck, between the superficial and deep layers of the cervical fascia. The borders of the posterior triangle are the sternocleidomastoid anteriorly, the trapezius posteriorly, and the clavicle inferiorly. It is here in the subcutaneous tissue that the nerve is in contact with the cervical lymph node chain. It then gives off several branches to the upper part of the trapezius muscle before passing under its anterior edge.8 In the trapezius muscle substance, the nerve continues obliquely as it innervates the lower part of the muscle. It then
descends parallel and medial to the vertebral border of the scapula,24 terminating in the trapezius musculature.
descends parallel and medial to the vertebral border of the scapula,24 terminating in the trapezius musculature.
DIAGNOSIS
Trapezius paralysis is frequently misdiagnosed at the initial presentation.3,4,37 Secondary effects of trapezius dysfunction, such as subacromial impingement, adhesive capsulitis, thoracic outlet syndrome, spasm of the other periscapular muscles, and paresthesias from traction on the brachial plexus, may cloud the diagnosis. Other diagnoses, such as stroke, shoulder dislocations, scoliosis, herniated disks, and progressive neuromuscular disorders, may present with symptoms similar to those of trapezius paralysis and should be ruled out.3,27,37 However, a detailed patient history and a thorough and careful examination will typically lead to the correct diagnosis.
History
The evaluation at the initial patient presentation begins with a complete medical history. Any recent illnesses, medical problems, history of trauma to the shoulder or neck, or any recent surgical procedures in this area should be elicited, especially in relation to the onset of the current dysfunction. Any deficit caused by traumatic injury to the spinal accessory nerve does not typically become obvious until several days after the initial swelling and pain have subsided. It is then that it becomes apparent that function is abnormal. If the nerve has been injured because of a minor surgical procedure in the area of the posterior cervical triangle, periscapular pain usually develops within several days.4 The gradual onset of atraumatic weakness and lateral scapular winging should be an alert to investigate possible neurologic or myopathic diseases.31
Most patients experience pain with prolonged use of the shoulder, as the other muscles strain and fatigue from overcompensation. This strain often causes significant muscle spasm that adds to the disabling pain some experience.4 Many also complain of a constant dull ache and heavy feeling about the shoulder. As the condition becomes chronic, the pain may radiate to the hand and forearm, to the face and head, and even to the contralateral extremity.6,34 As the shoulder droops inferiorly because of the fatigued compensatory muscles, the brachial plexus is placed under tension.3 This can lead to recurring episodes of radiating pain and paresthesias because of the traction effect, especially when the involved extremity has been unsupported in the early part of treatment.37 Abnormal scapular rotation, resulting from failure to rotate the scapula out of the way, may cause significant signs of impingement as the greater tuberosity abuts the acromion. This may also be the underlying cause of other associated symptoms such as glenohumeral instability, acromioclavicular joint incongruity, and adhesive capsulitis.33 Patients experience pain and difficulty with most all overhead activities, lifting heavy objects, prolonged writing, or driving a car.3 Unfortunately the pain is so disabling for some that chronic use of narcotic analgesics is necessary.3,4
Physical Findings
The physical examination begins with a thorough inspection, which requires males to remove their gown and females to fasten the gown just above the breasts. The examiner can then evaluate the general appearance, posture, and positioning of the extremity. It is important to look for scars, especially in the posterior cervical triangle. It is not infrequent for patients to have forgotten to mention seemingly insignificant past operations, such as lymph node biopsy. The neckline is asymmetric because the trapezius is atrophic on the affected side, which also slopes dramatically (Fig. 32-2). The shoulder droops as the scapula is translated laterally and rotated downward. The patient should be asked to actively elevate both arms in the forward plane, as the relationship
between the scapula and chest wall is observed; 80% of patients have no more than 90 degrees of active abduction, which is generally weak against resistance (Fig. 32-3). Patients will usually be unable to shrug the shoulder, although the levator scapulae can sometimes elevate the scapula enough to mask the shrug deficit.14 Lateral scapular winging is especially apparent against trapezius muscle resistance (Fig. 32-4). The weight duration test of Neer assesses the onset of fatigue and pain as the patient holds a heavy object at arm’s length.33
between the scapula and chest wall is observed; 80% of patients have no more than 90 degrees of active abduction, which is generally weak against resistance (Fig. 32-3). Patients will usually be unable to shrug the shoulder, although the levator scapulae can sometimes elevate the scapula enough to mask the shrug deficit.14 Lateral scapular winging is especially apparent against trapezius muscle resistance (Fig. 32-4). The weight duration test of Neer assesses the onset of fatigue and pain as the patient holds a heavy object at arm’s length.33
Related posts:
 Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Anterior Superior Rotator Cuff Tears: Repairable and Irreparable Tears
Arthroscopic Repair of Rotator Cuff Tears
Massive Tears of the Posterosuperior Rotator Cuff
Acute Fractures, Malunions, and Nonunions of the Clavicle
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Three-Part Fractures: Open Reduction and Internal Fixation, or Arthroplasty?
Anterior Superior Rotator Cuff Tears: Repairable and Irreparable Tears
Arthroscopic Repair of Rotator Cuff Tears
Massive Tears of the Posterosuperior Rotator Cuff
Acute Fractures, Malunions, and Nonunions of the Clavicle
Arthrodesis and Other Salvage Procedures: When Arthroplasty Is Not Indicated
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


