Fig. 2.1
Modern sport climbing, protected with bolts (Isabelle Schöffl in Dream Catcher, Laos 7b+)
Bouldering is defined as ropeless climbing involving a short sequence of powerful and technical moves to complete a graded route, or a sequence of few climbing moves, on large boulders, occasionally up to 10 m high.
Bouldering (Fig. 2.2) can be performed solo, without a partner, and with minimal equipment – climbing shoes and crash pad (a foam mattress designated to stop ones’ fall). Falling onto one’s feet or body is common in bouldering, whether a route is completed (defined as “topped”) or not.

Fig. 2.2
Boulderer and protection (for protection, a bouldering mat (crash pad) is used)
Traditional (alpine) climbing (or trad climbing) emphasizes the skills necessary for establishing routes in an exploratory outdoor environment. The lead climber typically ascends a section of rock while placing removable protective devices where possible and desirable along the climb. Falls can therefore be longer than those experienced when sport climbing. Unreliable fixed pitons may occasionally be found on older established routes. As physical hazards are likely, the use of a helmet is considered mandatory. If climbing is performed at an altitude of greater than 2,500 m, physiological altitude-induced adaptations must also be factored into the climb.
Indoor climbing is performed on artificial structures that try to mimic climbing outdoors but in a more controlled environment. As physical hazards are almost totally eliminated, climbing became a popular extracurricular school sport in many countries. National and international competitions are held on such walls and involve three major disciplines – lead climbing (i.e., sport climbing), speed climbing, and bouldering. Indoor bouldering is performed above thick foam mat flooring.
Ice climbing (Fig. 2.3) normally refers to roped and protected climbing of features such as glaciers, frozen waterfalls, and cliffs or rock slabs covered with ice refrozen from flows of water. Equipment includes ice axes and crampons. Physical hazards such as avalanches and rock and icefalls or breaks are present [3].

Fig. 2.3
Ice climbing (Sam Lightner on The Pencil, Polar Circus, WI6, Alberta, Canada)
Many different climbing grading systems exist, the most common of which are the Union Internationale des Associations d’Alpinisme (International Climbing Federation) UIAA, the French, and the Yosemite Decimal System scales. For scientific analysis, the decimal UIAA scale is recommended (Table 2.1) [5].
Table 2.1
The UIAA metric, the French, and the Yosemite Decimal System scales of climbing grades [5]
Metric scale | UIAA | French (Fr) | US-American (YDS) |
|---|---|---|---|
5.66 | 6− | 5b/c | 5.8 |
6 | 6 | 5c/6a | 5.9 |
6.33 | 6+ | 6a/6a+ | 5.10a |
6.66 | 7− | 6a+/b | 5.10b/c |
7 | 7 | 6b/b+ | 5.10d |
7.33 | 7+ | 6b+/6c | 5.11a/b |
7.66 | 8− | 6c+ | 5.11c |
8 | 8 | 7a | 5.11c/d |
8.33 | 8+ | 7a+/7b | 5.12a/b |
8.66 | 9− | 7b/7b+ | 5.12b/c |
9 | 9 | 7c/7c+ | 5.12d |
9.33 | 9+ | 7c+/8a | 5.13a |
9.66 | 10− | 8a/8a+ | 5.13b/c |
10 | 10 | 8b | 5.13d |
10.33 | 10+ | 8b+/8c | 5.14a/b |
10.66 | 11− | 8c/8c+ | 5.14b/c |
11 | 11 | 9a | 5.14d |
11.33 | 11+ | 9a+ | 5.15a |
11.66 | 12− | 9b | 5.15b |
Lead climbing means that the leading climber attaches himself to a dynamic climbing rope and ascends the route while periodically placing protection consisting of metal wedges or bolts temporarily placed into cracks in the rock face or “quickdraws” to bolts and attaching them to the climbing rope with carabiners. Top-rope climbing refers to climbing with a rope, used for the climber’s safety and runs from a belayer at the foot of a route through one or more carabiners connected to an anchor at the top of the route and back down to the climber, usually attaching to the climber by means of a harness.
Injury and Fatality Risk
Traditional Climbing, Sport Climbing, and Bouldering
From a cross-sectional survey, Schussmann [6] concluded that rock climbing has a lower injury rate than football and horse riding; however, these sports rarely result in catastrophic events or fatalities. Climbing frequency and difficulty are associated with the incidence of overuse injuries in most studies [7, 8]. Most injuries are sustained by the lead climber, with falls being the most common source of acute injuries [9]. Repeatedly performing hard moves is the most common cause for overuse injuries [8]. In traditional climbing, falls resulting in wall or ground strike lead to most injuries, while in the safer discipline of sport climbing, performing strenuous moves tends to be the leading cause of injury. Overall, the majority of injuries described in climbing studies are of minor severity, with a fatality rate ranging from 0 to 28 % [3]. Given the range of mortality rates, it is understandable that differing methodology and data collection techniques exist, which makes direct comparison between series difficult.
Indoor Climbing
Of all climbing subdisciplines, indoor climbing reports 0.027–0.079 injuries per 1,000 h of participation and very few fatalities [3]. However, overuse injuries of minor severity predominantly involving the upper limbs, mainly the fingers, are commonly reported in rock climbing studies.
Ice Climbing
Ice climbing popularity is growing fast, while very little data on injuries and accidents exist for this subdiscipline. The overall injury rate published in the literature is comparable with other outdoor sports (2.87–4.07 injuries/1,000 h [3, 10]), with most injuries of minor severity. Nevertheless, objective danger is always present, and severe injuries and fatalities do occur [3, 10].
Mountaineering
Mountaineering also involves a wide range of activities, from hiking up to climbing peaks above 8,000 m. All these activities present different physiological demands and risks depending on climbing style, altitude, environmental conditions, climbing experience, and more [11]. Most studies on mountaineering fatalities and accidents are giving the fatality/accident number per 1,000 climbers or per 1,000 summits, which are therefore difficult to compare to the 1,000 h of sports performance used in other disciplines. For higher altitude, not only the accident and fatality rate is important but also the prevalence of altitude illness, which is between 28 and 34 % above 4,000 m [12, 13]. These illnesses can be a contributing factor to an injury, accident, or death. They are characterized by shifts of internal body fluid, being in places they should not be on exposure to altitude (i.e., brain, lungs). At “high altitude” (5,000+ m), there is a risk that these altitude-induced internal fluid shifts may accumulate in the brain (high-altitude cerebral edema – HACE) and/or in the lungs (high-altitude pulmonary edema – HAPE). Both HAPE and HACE are potentially fatal [12].
When assessing climbing risks, it is obvious that each climbing subdiscipline would determine different levels and types of risk, injury, and fatality. When climbing outdoors, there are objective dangers and physical hazards: variable rock and ice quality, extreme and changing weather conditions, weapon-like equipment (ice climbing), difficult approaches, and high mental and physical stress. In mountaineering, additional environmental factors (avalanches, crevasses, altitude-induced illnesses with neurological dysfunction, etc.) can sometimes directly influence injuries and fatalities [11]. Nevertheless, dangerous situations and predictable injury patterns or accident circumstances can still be avoided or successfully managed with adequate preparation, training, and experience. In contrast, in indoor and sport climbing, these objective and external dangers are greatly reduced, although the risk of a fatal injury is still present.
Equipment
In the early days of climbing, classic heavy mountaineering boots were worn for climbing in alpine regions as well as in rock faces. It was only in the early 1980s when the first real, or modern, climbing shoe with a friction sole was introduced. One common characteristic which all climbing shoes share is the tight, squeezed fit required to obtain optimal contact with the rock. This excessively tight footwear leads to foot problems, such as callosity, toenail infections, or, in a longer term perspective, a hallux valgus deformity [14]. The introduction of predrilled anchoring bolts was an important factor for the explosive development of the climbing grades scaled. Lead climber falls, relaying on the rope and anchoring bolts, are common for sport climbers now. The climbing harnesses used have improved. While a combination of chest and sit harness has been used in traditional mountaineering, a pure sit harness design is now used in sport climbing. This allows maximum free movement while climbing and aims to reduce injury when falling [9, 15]. Bolts, ropes, harnesses, and other equipment used should carry the UIAA Safety Commission approval.
Ice climbing equipment also developed a long way from the tools used in classical mountaineering. Modern crampons with the prominent frontal spikes have initially become popular when Anderl Heckmaier and Wiggerl Vörg used them for the first ascent of the Eiger North Face. Nowadays, a single frontal spike or a heel spur is considered a state-of-the-art. Ice axes were already in use at the time of the first ascent of the Mont Blanc by Pascard and Balmat on 8 August 1786 and have evolved remarkably since. Recent technological advances have helped to transform these long-shafted tools into a short-shafted curved and surprisingly light crossbar that resembles a mythical medieval weapon. It is a topic of wide and hot discussion in the ice climbing community whether ice axes should be used with or without a leash. Leashes attach the ax to the climber’s wrist, reduce stress onto the forearms, but increase the risk of injuring oneself from the ax during a fall where typically the ax bounces back into the climber’s face. In parallel with the technological advancements in crampons and ice axes, Erich Friedli from Switzerland developed the first real ice screw [10]. This ice screw has played a pivotal role in increasing the safety of the sport. If placed correctly, in good ice and proper angle, it may guarantee a comparable pullout strength to bolts. All climbing disciplines use climbing ropes for protection. These ropes are dynamic ropes, in contrast to static ropes as used in sailing and caving. Dynamic ropes have a stretch of roughly 5 m per 50 m when stressed, which reduces the force onto the falling climber’s body.
Training in Rock Climbing
The recent increase in levels of technical difficulty in rock climbing has intensified the impacts of the sport onto the musculoskeletal system. The age of the top athletes, especially in competition climbing, has steadily decreased. In 1986, the average competitive member of the German National Climbing Team spent about 10 h per week training and was 26 years old. By 1996, the competitive climber was spending 21 h a week training and his/her age had dropped to 22 years [2]. Today it is not uncommon for 50 % of World Cup finalists to be under 18 years old. In this age, the finger phalanges’ growth plates have not fully closed yet in some of these young strong climbers, which frequently leads to unusual epiphyseal fatigue injuries [16]. While the majority of climbing activity and training is performed on rock or artificial climbing walls, certain climbing-specific training forms must also be considered. One of the most specific isolated and designated training forms is “to campus” (Fig. 2.4).
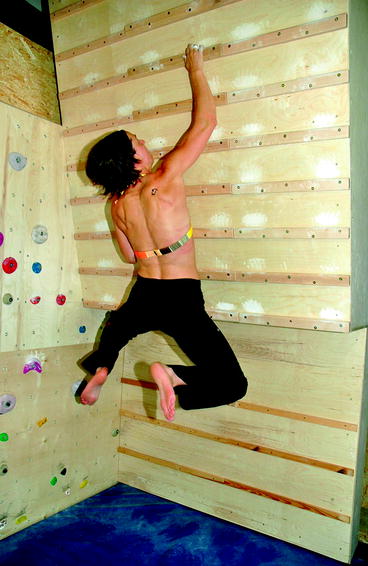
Fig. 2.4
Campus board training
The legendary “campus board,” built by Wolfgang Güllich and Kurt Albert at the Nuremberg “campus” gym, has become a household term among climbers. By training on the campus board, both in a positive and negative slope, Wolfgang developed his finger and forearm strength for the first ascent of “Action Directe” (the world’s first UIAA 11/5.14d, in Frankenjura, Germany). The campus board is a slightly overhanging board with different-size rungs in a constant pattern screwed onto it. Basic exercises contain climbing up and down hand over hand without feet, increasing the distance between the rungs used. A special training technique is “double dynos.” Based on the training principle of “plyometric training,” the climber jumps up and down from small-sized rungs. This applies very high forces onto the fingers and, respectively, onto the ligaments, bones, and cartilage. While “campusing” is a good training exercise in the elite ranks, it should have no place in training of beginners, intermediates, and especially preadolescent climbers! According to the author’s experience, two-thirds of junior climbers who trained regularly on the campus board sustained an injury! These injuries, commonly epiphyseal fatigue fractures, lead, if neglected, to a permanent damage of the affected finger. As a result, the main focus in the education of trainers, climbing instructors, parents, and young climbers should be focused on proper training methods and avoiding, as much as possible, techniques which may lead to these well-described injuries.
Injuries and Overuse Syndromes
While climbing relies on the synchronized and optimal function of the whole body, activity and performance are primarily limited by finger and forearm strength. The various gripping techniques (mostly crimp and hanging grip) (Figs. 2.5 and 2.6), which are used by the climber, led to the transmission of extremely high forces in the anatomical structures of the fingers. As a logical consequence, finger and hand injuries, predominantly overuse syndromes, are the most common complaints in rock climbers [7, 8, 17, 18]. A study evaluating 604 injured rock climbers found that 247 (41 % of injuries) sustained finger injuries (Table 2.2) [19, 20]. Some injuries, such as flexor tendon pulley ruptures or the lumbrical shift syndrome, are very unique and specific for the sport of climbing and are rarely seen in other patient populations [7]. As a result of this, it can be difficult to establish a diagnosis in uncommon and yet characteristic injuries for the general physician unfamiliar with climbing injury patterns (Table 2.3).

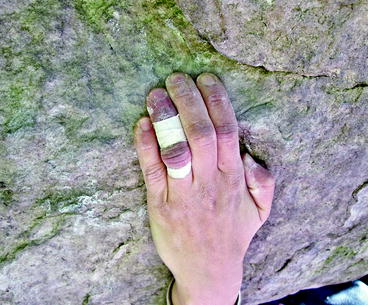
Figs. 2.5 and 2.6
The crimp and the hanging grip technique are common climbing finger holds involving very small rock face ledges or slopes which the climbers is holding to
Table 2.2
The ten most frequent localization of climbing-specific diagnoses 1/98–12/01 (n = 604) [20]
Fingers | 247 | (41.0 %) |
Forearm/elbow | 81 | (13.4 %) |
Foot | 55 | (9.1 %) |
Hand | 47 | (7.8 %) |
Spine/torso | 43 | (7.1 %) |
Skin | 42 | (6.9 %) |
Shoulder | 30 | (5.0 %) |
Knee | 22 | (3.6 %) |
Others | 37 | (6.1 %) |
Polytraumatic | 5 | (0.8 %) |
Diagnosis | N out of 271 | Acute onset | Slow onset | Chronic onset |
|---|---|---|---|---|
Pulley rupture | 74 | + | + | |
Pulley strain | 48 | + | + | |
Tenosynovitis | 42 | + | + | + |
Joint capsular damage and ligamental injuries | 37 | + | + | |
Arthritis (acute) | 13 | + | + | |
Ganglion | 11 | + | + | + |
Flexor tendon strain | 7 | + | ||
Fracture | 7 | + | ||
Arthritis (chronic) | 7 | + | ||
Dupuytren contracture | 5 | + | ||
Soft tissue injury, contusion | 5 | + | ||
Flexor tendon partial tear | 4 | + | ||
Collateral ligament injury | 3 | + | + | |
Osseous tear fibrocartilago palmaris | 2 | + | ||
Epiphyseal fracture | 2 | + | + | |
Lumbrical shift syndrome | 2 | + | + | |
Abscess/cellulitis | 1 | + | ||
Finger amputation | 1 | + | ||
Tendon nodules | + | |||
Joint contracturea | + | |||
Finger nerve irritation | + | |||
Extensor tendon irritation | + | + |
Clinical Examination and Diagnostics of Finger Injuries
A climber’s injured finger, or a relevant complaint, requires a careful history, precise examination, and directed imaging. Both the active and passive range of motion of the proximal (PIP) and distal (DIP) interphalangeal joints should be measured. It is essential to examine the flexor tendons separately by isolating flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) function. The collateral ligaments of the finger joints should be assessed through the application of lateral stress and the palmar plate through the translation test, which is analogous to Lachman test on the knee joint. For detection of a pulley rupture, an opposition of the injured finger against the thumb with forceful pressing in the crimp position may lead to a palpable or visual bowstring. Pressure tenderness on the palmar side of the base phalanx is present in both pulley rupture and tenosynovitis, while tenderness on the phalanges’ side usually implies a lumbrical muscle injury.
High-energy acute injuries as well as any type of chronic problem require a radiograph in two planes. Further diagnosis may be provided by ultrasound, e.g., in detecting a pulley injury, ganglions or tenosynovitis of the fingers, biceps inflammations, or rotator cuff problems. The technique of finger ultrasound is easy to learn and is very accurate and cost-effective. A linear array transducer with 10–12 MHz in a prone position performing longitudinal and transversal planes is mostly used. For signal enhancement, a gel standoff pad or examination in a warm water basin is recommended. Only in rare cases an additional MRI (or CT) needs to be performed in order to establish a clear diagnosis. In some cases, electromyography might be indicated when localized atrophy is suspected. That would be appropriate in nerve traction injury such as with suprascapular or long thoracic nerve for winging scapula.
Normal Musculoskeletal Adaptations in the Climber’s Body
The high stresses involved in rock climbing, specifically at the fingers, lead to physiologic adaptations over the years, which need to be distinguished from pathologic changes. Through radiographic and MRI analysis, Hochholzer et al. [21] demonstrated the presence of these adaptations. They found an adaptive hypertrophy of the joint capsule, thickening of the collateral ligaments, cortical hypertrophy, and a hypertrophy of up to 50 % of the flexor tendons itself. The authors hypothesized that cortical hypertrophy could be adaptive signs to the high stress of the sport and not already pathological osteoarthrotic changes [22, 23]. Therefore, clinical and radiographic findings must be carefully interpreted. In an analysis of radiographs in young high-level climbers and 140 experienced climbers, Schöffl et al. [23] classified the following findings under the definition of a stress reaction: cortical hypertrophy, subchondral sclerosis/increased thickness of epiphysis, calcifications of the insertion of the flexor digitorum superficialis or the flexor digitorum profundus tendon, and broadened proximal and/or distal interphalangeal joint base (Table 2.4).
Table 2.4




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
