Revision Total Knee Arthroplasty via Tibial Tubercle Osteotomy
Patient Selection
Number of total knee arthroplasties (TKAs) increased in past 20 years; projected to reach 3.5 million primary and 268,000 revision cases by 2030
Quadriceps snip and tibial tubercle osteotomy (TTO) were developed to improve exposure in revision TKA (rTKA) as well as complex primary TKA
Most patients are managed with quadriceps snip; surgeon may opt for a TTO early to avoid being forced into a secondary TTO after quadriceps snip fails
Indications
Rigid, severe lack of range of motion (ROM); consider for ROM less than 90° of flexion, especially with severe fibrous block in motion
May be necessary during rTKA for two-stage exchange for infection, stiff/painful primary TKA, and neglected aseptically loosened TKA
Contraindications
Poor bone stock in proximal tibia
Can be overcome by extending TTO segment further distally into tibial diaphysis
Preoperative Imaging and Evaluation
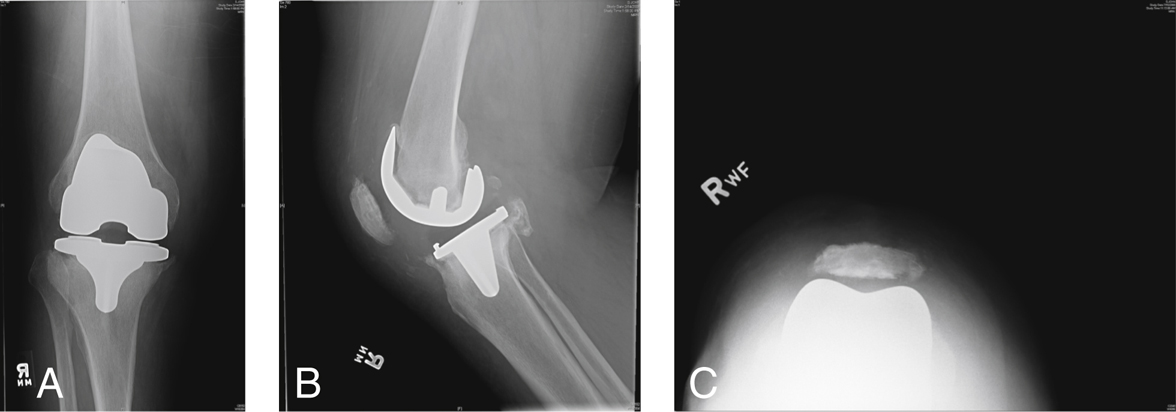
Figure 1Weight-bearing AP (A), lateral (B), and sunrise (C) radiographs of the knee of a patient who underwent a total knee arthroplasty (TKA) 1 yr earlier. The TKA was revised for pain and stiffness.
AP weight-bearing, lateral, sunrise radiographs (Figure 1)
Physical examination, specifically preoperative ROM
Procedure
Room Setup/Patient Positioning
Standard supine positioning for TKA
Excessive external rotation can be minimized with a padded bolster under the ipsilateral hip and/or a padded hip positioner placed lateral to the tourniquet
Special Instruments/Equipment/Implants
Full set of straight and curved osteotomes
Motorized microsagittal saw
18-gauge stainless steel wires, 2.7-mm drill bit, wire tightener, or 6.5-mm cannulated screws. The authors prefer wires as they are lower profile and less likely to cause fracture through the osteotomized fragment
 | Video 65.1 This video segment shows a tibial tubercle osteotomy performed in an elderly patient undergoing rTKA for chronic pain and stiffness. Jeffrey A. Geller, MD. (2 min 30 s) |