Sam’s practitioner has now identified several issues that Sam is facing, and she and Sam have been working on several of them over the last 3 months. They are making progress together, but today Sam said he was feeling frustrated about not achieving more.
Sam’s rehabilitation practitioner is struck by how many issues she and Sam have identified, and feels confused about how to proceed. It is time to take stock, prioritise the remaining issues, and revise the rehabilitation programme. She decides to make a summary, and try to see how the issues may relate to each other.
On readministration of the HoNOS (see Chapter 3), Sam’s acute symptoms, social withdrawal and problems with self-care have now resolved, and after doing weekly cognitive remediation (see Chapter 9), his concentration and memory are much improved. However, he has some problems getting to sleep (often awake until 2–3am, also often sleeping in the afternoons), motivation, emotional responsiveness and lack of pleasure. There was a question of whether his medication was contributing to his fatigue, lack of energy and restlessness; recent medication reductions he negotiated with his psychiatrist do seem to have reduced these problems (as confirmed by readministration of the LUNSERS (see Chapter 3). He continues to take his medication daily (with occasional lapses), despite being dissatisfied with the side-effects.
As his acute symptoms resolved, insight into his problems and awareness of their impact on his life appeared to worsen his dysphoria. He expressed a lack of confidence in being able to address functional challenges, and this thought (together with his belief that his life was destroyed) appeared to both be exacerbated by dysphoria and to contribute to it continuing. After some weeks with very high levels of distress, his Kessler-6 score has recently been much improved (see Chapter 2), although it remains in the clinical range. Sam says that he found fun activities did make a difference (see Chapter 8) but he found it hard to keep going. In particular, he started practising the guitar again for a time, but he has not touched it now for 4 weeks. Nor has he been very physically active over the last 6 weeks (see Chapter 13).
After a motivational interview (see Chapter 6), Sam attempted to stop smoking. This attempt lasted 5 weeks, ending after an argument with his girlfriend, Angela, over her missing her own medication doses. He went out drinking, and accepted a cigarette from someone at the bar, and is now smoking as much as before.
Sam went to a group session at the centre about his drinking (see Chapter 13) but at the time, his social anxiety was too high to continue. Instead, he did some segments of an internet-based alcohol intervention on one of the centre’s computers (see Chapter 16), with occasional help from one of the staff. Apart from the incident when he returned to smoking, he has only been drinking 1–2 times a week, and has not had more than two drinks (20 g ethanol) on any occasion (see Chapter 2).
Sam completed the centre’s group social skills programme (see Chapter 11), including segments on writing a resumé and fielding interview questions: his social performance is now considerably better than when he started at the centre, and he no longer has significant social anxiety. He has even started participating in an online peer support programme one or twice (see Chapter 14).
Sam also completed a programme on transportation (see Chapter 12) and now has no difficulty using public transport. He attended some cooking lessons at the rehabilitation centre, but Angela still does most of the cooking.
He obtained an evening job as a cleaner, and both his mood and sleeping improved. However, he lost the job after a week, when he did not turn up for work on two successive evenings (he said he was tired, after working on Angela’s car during the day). Financial worries continue, and he still has some problems managing a budget (see Chapter 12). This remains a source of conflict with Angela.
Sam is now staying overnight at Angela’s flat more than he is at home. This has reduced the tension at home to some extent, but Sam’s mother still worries about him. She has usually been the first person to notice his episodes emerging, and it is usually she who approaches services for help. Sam becomes irritated by her questioning him about how he is feeling, and says she treats him like a child. Staying with Angela helps him to avoid his mother’s questioning.
Despite his achievements, Sam still lacks some optimism and a sense of control over the future on an Empowerment scale (see Chapter 4). Similarly, a readministration of a WHOQOL-BREF (see Chapter 5) shows that scores on psychological health and environmental quality of life remain low.
The complexity of this picture is not unusual. Nor is the fact that progress is patchy and is not always fully sustained. There is a risk that both client and practitioner might focus on what has not been achieved, rather than on positive achievements. Summarising those achievements can make an important contribution to the optimism and self-efficacy of both parties.
A case summary of this kind can also identify inter-relationships between issues, and changes that have (or could have) an impact on multiple important aspects of Sam’s life. An example of how this summary can be used is provided below.
Together with Sam, his practitioner makes a list of his achievements since they began working together (
Table 17.1).
Sam is amazed to see the list. ‘Wow! We have done quite a lot in 3 months, I guess. I hadn’t put it together.’ However, he still felt frustrated that he hadn’t been able to persist with some things. It felt like he had slipped back in many ways.
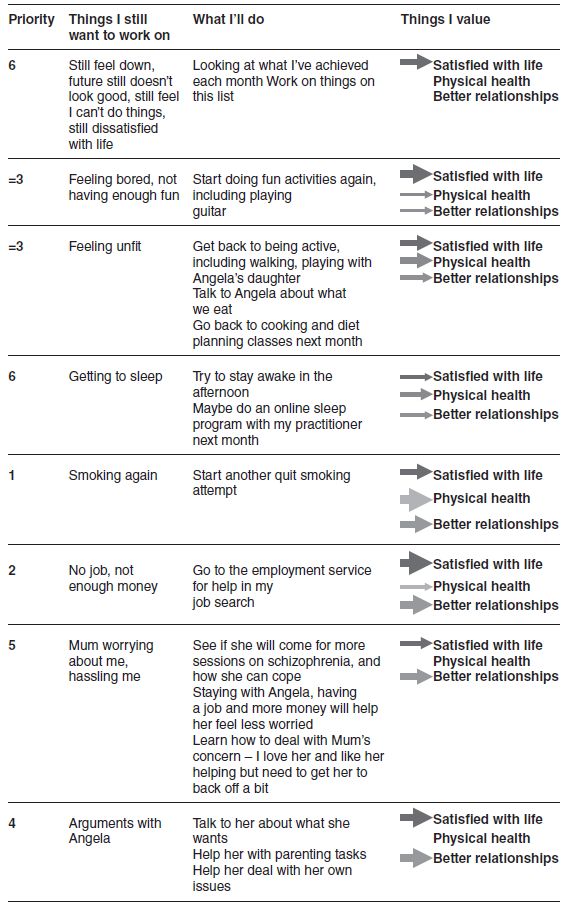
Sam’s practitioner suggests they make a list of things that may still need some attention (
Table 17.2, column 2). Then, they review the things that Sam values most – he now see them as satisfaction with life, physical health and better relationships (
Table 17.2, last column). They brainstorm some ideas about how they could work on remaining issues (
Table 17.2, column 3).
Table 17.1 Sam’s list of achievements.
|
Took medication regularly |
No more hallucinations or odd ideas, less unhappy |
Came to most rehab sessions and usually tried out ideas between sessions |
Some things are getting better |
Talked to doctor about medications (he cut the dose) |
Less restless and tired |
Looked after myself better (washed, shaved every day, wore deodorant, cleaned my teeth, went to the dentist) |
Now look/smell better |
Quit smoking for 5 weeks (!) |
Felt much healthier, more able to breathe when didn’t smoke. Fewer arguments with Angela |
Did computer training programme for my attention and memory (and remembered to come to most sessions!) |
Can concentrate and remember things better now |
Went to the social skills group, despite feeling anxious about it. Took part in a couple of online peer support sessions |
Less anxious around people, and mixing more. Can now write my CV and do a job interview |
Tried to play the guitar and do other fun things, was more active for about 2 weeks |
Less unhappy when I did them, felt fitter when I was active |
Went to a group session and did some work on a computer for my drinking. Cut down my drinking to 1–2 times a week, no more than two drinks (still doing it!) |
A bit more money, feel better the next day |
Went to two cooking classes |
Could cook a potato, make a hamburger after the classes (not sure I still can) |
Finished a transport group |
Can catch the bus to the supermarket and the city |
Got a cleaning job for a few days |
More money that week |
Kept seeing Angela, told her I love her, made up after arguments |
Relationship with Angela has now lasted 3 months – the longest ever |
When faced with many issues, it is often hard to know where to start. We recommend that readers give this question some thought before carrying on to see what Sam’s practitioner does. It is likely that different practitioners and clients may come to different conclusions about how to proceed, and there may be many directions that could lead to positive outcomes. It can be helpful to discuss ideas with the rehabilitation team to obtain others’ perspectives, and then take some of the discussion points back to the client.
Some considerations that help with this process include the following.
- What is most important to the client? In particular, what links most closely to their core values (see Chapter 7)?
- What is most urgent?
- What is a focus that will be likely to give early gains and build confidence?
- What things may impact on multiple areas, so that widespread gains are obtained?
Table 17.2 Sam’s list of things he still wants to work on.
< div class='tao-gold-member'>