Abstract
Objectives
Isokinetic assessment is currently the reference method for measuring dynamic muscle strength. We have sought to evaluate the reproducibility over time of isokinetic testing of the hip flexor (FI) and extensor (Ext) muscles and to establish whether there is a significant difference in peak torque (PT) between the left and right hips.
Patients and methods
Ten adults were tested once a week for 3 weeks by the same investigator and according to the same protocol, with two velocities (60°/s and 180°/s) for the hip FI and Ext in concentric tests and one velocity (30°/s) for the Ext only in eccentric tests. The reproducibility of the measured PT was analyzed by using the intraclass correlation coefficient (ICC) and a Bland and Altman plot. The difference in PT between the right and left hips was tested using Student’s T test.
Results
The ICC for the observed PT values revealed very good reproducibility (with a value of between 0.75 and 0.96) for the hip FI and Ext measurements (regardless of the body side, test velocity or contraction mode). We did not observe any significant PT differences between the right and left hips.
Conclusion
The isokinetic assessment of the concentric and eccentric PT values generated by the hip FI and Ext is highly reproducible. There is no difference between dominant and nondominant body sides, which enables the use of the contralateral limb as a reference.
Résumé
Objectifs
L’isocinétisme est actuellement la méthode de référence pour mesurer la force musculaire dynamique. Nous avons étudié la reproductibilité des tests isocinétiques appliqués aux fléchisseurs (FI) et extenseurs (Ext) de hanche. Nous avons également étudié s’il existe une différence significative entre les hanches droites et gauches.
Patients et méthodes
Dix sujets ont été testés à trois reprises, à une semaine d’intervalle par le même examinateur, selon le même protocole : deux vitesses en concentrique pour les FI et Ext (60° par seconde et 180° par seconde) et une vitesse en excentrique pour les Ext uniquement (30° par seconde). La reproductibilité des moments de force maximum (MFM) a été étudiée par le coefficient de corrélation intraclasse (CIC) et la méthode graphique de Bland et Altman. La différence entre les hanches droites et gauches a été évaluée par le test t de Student.
Résultats
Les CIC des mesures du MFM montrent une bonne à très bonne reproductibilité (CIC de 0,75 à 0,96) pour les muscles FI et Ext de hanche indépendamment du côté, de la vitesse de test et du mode de contraction. Nous n’avons pas observé de différence significative entre les MFM des hanches droite et gauche ( p < 0,05).
Conclusion
La mesure isocinétique du moment de force maximum (MFM) des FI et Ext de hanche en mode concentrique et excentrique présente une bonne reproductibilité. Dans cette population de sédentaires et sportifs de loisir pratiquant des sports symétriques, on ne note pas de différence entre les groupes musculaires homo- et controlatéraux ce qui autorise l’utilisation du membre controlatéral comme référence.
1
English version
1.1
Introduction
Methods for evaluating hip muscle strength are scarce and have only been partially validated to date . Hip flexor (FI) and extensor (Ext) muscle strength can be measured by using various contraction modes, which can be either isometric or anisometric. Within the latter class, one can distinguish between constant-load exercises (isotonic contraction) and constant-velocity exercises (isokinetic contraction). The isokinetic mode enables muscle strength to be assessed and quantified under more natural movement conditions than the isometric method does.
The hip’s main FI muscles are the iliopsoas and the rectus femoris. The function of the iliopsoas depends on the fulcrum point: it can generate thigh flexion (relative to the pelvis) if the fulcrum point is proximal or lumbar hyperlordosis if the fulcrum point is distal. The rectus femoris is the only two-joint muscle in the quadriceps group: it becomes fully stretched when hip extension is combined with knee flexion. The hip’s main Ext muscles are the gluteus maximus and the hamstrings. The latter are two-joint muscles and bridge the hip joint (acting as hip Ext) and the knee joint (acting as knee FI). Hence, a flexed-hip, extended-knee position (with the hamstrings fully stretched in the starting position) may expose the subject to the risk of injury. This parameter has a major impact on the choice of the knee joint position during isokinetic testing of the hip Ext.
Isokinetic testing is known to be reproducible for the knee , shoulder and spinal joints. However, studies of the hip joint are scarce and sometimes contradictory; although Dugailly reported good reproducibility values for all the hip muscles (apart from the abductors), Emery et al. noted poor reproducibility for the FI and adductors at high velocities. Most reproducibility studies have been performed with the subject in the lying position . The subjects were healthy adults in most studies, with the exception of Burnett et al.’s work on children aged from 6 to 11. Three studies have adopted much the same methodology, with concentric-mode evaluation of the reproducibility of the hip FI and Ext at low (30 to 60°/s) and high (90 to 120°/s) velocities. The values of the intraclass correlation coefficients (ICC) in these studies ranged from 0.63 to 0.94, which corresponds to moderately good to very good reproducibility. The study by Emery et al. was particular in that it only investigated the hip FI during the execution of alternating concentric and eccentric movements at test velocities of 60°/s and 150°/s. The reproducibility was poor to moderate, with ICC values less than 0.68. One only study has looked at reproducibility in the standing position (Guskiewicz et al. ). Concentric-mode tests were performed on the hip FI alone, at velocities of 60 and 240°/s. The ICC values ranged from 0.82 to 0.96 (i.e. good to very good reproducibility).
There are many types of isokinetic dynamometers on the market; literature studies using different machines are thus difficult to compare directly; Dugailly used a Cybex ® , whereas Arokoski et al. used a Lido ® . The recently launched CON-TREX ® MJ dynamometer (CMV AG, Zürich, Switzerland) has many technical advantages: easier positioning, the ability to program different contraction modes during a single test session (concentric movement during extension and eccentric movement during flexion, for example), the presence of a gravity compensation mechanism for patients with muscle strength values of around 3 out of 5 on the Medical Research Council (MRC) and rehabilitation modes with visual feedback.
Furthermore, the issue of leg dominance is also subject to debate: although Tippett reported dominance in baseball pitchers, Alexander , Smith et al. , Calmels and Dugailly did not find this type of effect. The lack of dominance may enable the use of the contralateral hip as a reference.
The primary objective of the present study was to evaluate the intraobserver reproducibility of isokinetic measurement of the peak torque (PT) generated by the hip FI and Ext muscles with the subject in the supine position, at different angular velocities and in concentric and eccentric movement modes.
The study’s secondary objective was to compare the PT values for each leg and establish whether or not a dominance effect was present.
1.2
Patients and methods
1.2.1
Study population
Ten healthy, adult volunteers (nine men and one woman) participated in the study. All were either sedentary or participated in recreational sporting activities and were not suffering from leg injuries or limb disorders. The subjects gave their informed, written consent to participate and were not paid an honorarium.
1.2.2
Sample size calculation
On the basis of preliminary data from four subjects, we considered that a minimum ICC of 0.65 would be acceptable (H0: ρ 0 = 0.65) and predicted that an ICC of at least 0.9 would be observed (H1: ρ 1 = 0.90). The type I and type II errors were set to 5% and 20%, respectively. Using the method described by Walter et al. , the number of subjects required to detect an ICC of at least 0.65 is around 10, as long as three series of muscle strength measurements are performed.
1.2.3
Protocol
The tests were performed on a CON-TREX ® isokinetic dynamometer (CMV AG, Zürich, Switzerland). The subject lay in the supine position with the hip in the sagittal plane and the knee flexed at 90°. We chose the horizontal (lying) position because it appears to yield more reliable measurements (notably by limiting compensations). The contralateral leg rested on (but was not attached to) a support under the foot, with 0° of hip extension and the knee flexed at 90°. The dynamometer’s axis was aligned with the trochanter major (corresponding to the axis of hip flexion/extension). The subject’s body was held by a strap around the pelvis (over the anterior superior iliac spines) and one chest belt. The test leg was attached to the dynamometer via a thigh strap ( Figs. 1 and 2 ). The test started with an extension movement.


Gravity correction was always performed during the pretest calibration phase.
Three tests were performed at 7-day intervals by the same investigator and with the subject in the same position each time.
The evaluation was performed with a joint amplitude of 90° (from 10° of hip extension to 80° of flexion) in concentric-mode movement for the Ext and FI and in eccentric-mode movement for the Ext only.
After a 5-min warm-up on a cycle ergometer (power setting: 1 Watt/kg), the subject lay on the dynamometer and performed five sub-maximal practice contractions for each mode and at each velocity. The dominant side was always tested first.
For concentric testing, the subject performed four maximal contractions of the hip Ext and FI at a velocity of 60°/s and then five maximal contractions at a velocity of 180°/s.
For eccentric testing (performed on the Ext only), the subject performed four maximal contractions at 30°/s and then four maximal contractions at 90°/s. During this phase, the subject was told to keep his/her leg extended so that the hamstrings were the prime hip Ext involved in the exercise (since the hamstrings are two-joint muscles, knee extension meant that they were fully stretched in the starting position).
We selected the best rep from each series and took the PT as a measure of hip Ext and Fl strength. The PT was measured during assessments in week 1 (W1), week 2 (W2) and week 3 (W3).
1.2.4
Statistical analyses
The population was described in terms of the median and 25 th and 75 th percentiles (for quantitative variables) and the number and percentage (for qualitative variables). The PT was expressed in Newton metres (N.m).
1.2.4.1
Reproducibility analysis
The test-retest reproducibility was estimated according to two different methods.
The first method consisted in calculating the ICC for measurements of the left and right legs in W1, W2 and W3. The extent of agreement was considered to be very good for an ICC greater than 0.90, good for ICC between 0.90 and 0.70, moderate for ICC between 0.51 and 0.70 and poor for an ICC less than 0.51 .
For the analysis of fixed and proportional biases, we generated a Bland and Altman plot for the first two measurements (W1 and W2) .
1.2.4.2
Comparison of the right and left hips
For each subject, we calculated the difference between the right and left sides for each test (W1, W2 and W3). The mean difference was compared with the null value using a paired Student’s t test.
The level of statistical significance was set to p ≤ 0.05. All analyses were performed with SAS software (SAS Institute, Cary, USA).
1.3
Results
1.3.1
The study population
Ten subjects (nine males [90%] and one female [10%]) were included in the study. The median age was 30.5 (28.3–39.3), the median weight was 75.5 kg (69.3–78.0) and the median height was 173.5 cm (173.0–174.8).
1.3.2
Reproducibility of the measurements
1.3.2.1
Intraclass correlation coefficients
The ICC for the PT measurements (with values ranging from 0.75 to 0.96) revealed good to very good reproducibility for the hip FI and Ext muscles, regardless of the body side, test velocity and contraction mode ( Table 1 ). The only exceptions were the right hip Ext in low velocity, concentric tests (ICC: 0.62) and the left hip Ext in low velocity, eccentric tests (ICC: 0.68).
| Left hip | Right hip | |||
|---|---|---|---|---|
| ICC | Reproducibility | ICC | Reproducibility | |
| Con. extension 60°/s | 0.80 | Good | 0.62 | Moderate |
| Con. flexion 60°/s | 0.90 | Good | 0.94 | Very good |
| Con. extension 180°/s | 0.94 | Very good | 0.83 | Good |
| Con. flexion 180°/s | 0.94 | Very good | 0.96 | Very good |
| Ecc. extension 30°/s | 0.68 | Moderate | 0.80 | Good |
| Ecc. extension 90°/s | 0.75 | Good | 0.78 | Good |
1.3.2.2
Analysis of fixed and proportional biases
By using a Bland and Altman to study fixed bias , we found that despite good reproducibility, the measurements performed in W2 were almost always better than those performed in W1 (except for the right hip FI in high velocity concentric tests and the left hip Ext in high velocity, eccentric tests) ( Fig. 3 ). However, this difference between W2 and W1 is negligible with respect to the absolute values of the measured parameters (except for the right hip Ext in low velocity eccentric tests).
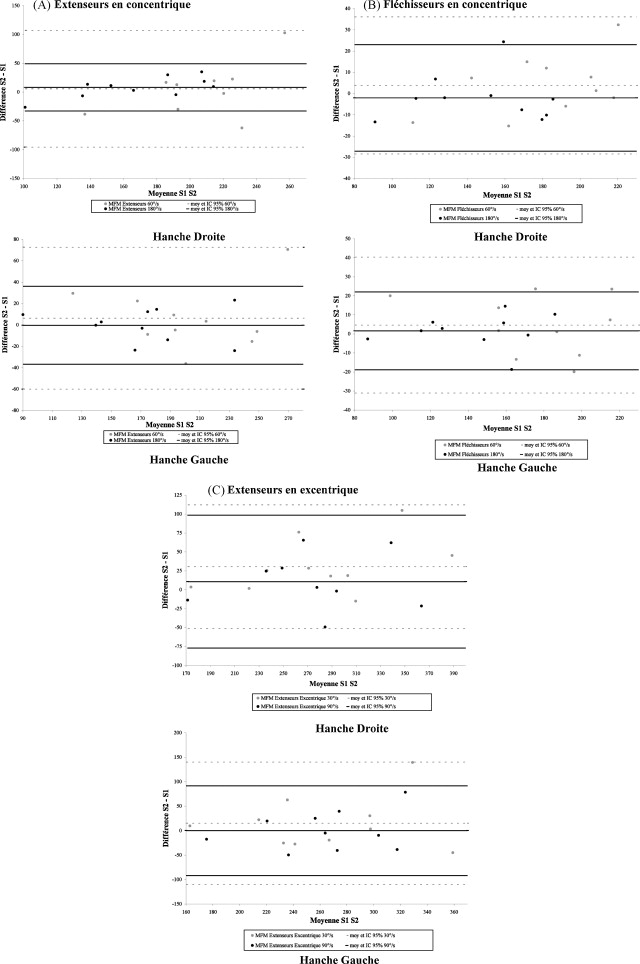
Analysis of the proportional bias with a Bland and Altman plot revealed that the PT value did not have a significant impact on the difference between W2 and W1. At best, we observed a slight trend towards greater differences between W2 and W1 with increasing PT values for the right hip Ext in concentric tests, the left hip FI in concentric tests and the left hip Ext in eccentric tests.
1.3.3
Comparison of the right and left hips
There were no significant differences between the respective PT values for the right and left hips at W1, W2 and W3, except for concentric flexion at 180°/s ( p = 0.02) in W1 (the median right/left difference was 5.8 N.m, for absolute PT values ranging from 150 to 250 N.m) ( Table 2 ).
| Week 1 | Week 2 | Week 3 | ||||
|---|---|---|---|---|---|---|
| MD R/L (q1–q3) | p | MD R/L (q1–q3) | p | MD R/L (q1–q3) | p | |
| Concentric extension 60°/s | 12.1 (−5.7; 28.3) | 0.30 | 3.3 (−2.4; 19.1) | 0.22 | 7.1 (−7.8; 12.8) | 0.60 |
| Concentric flexion 60°/s | 1 (−8.2; 13.1) | 0.36 | 4.8 (−4.5; 22.3) | 0.46 | 11.1 (0; 21.4) | 0.07 |
| Concentric extension 180°/s | −8.4 (−23.4; 17.3) | 0.54 | 4.35 (−17.2; 18.4) | 0.74 | 8.8 (−6.9; 17.6) | 0.89 |
| Concentric flexion 180°/s | 5.8 (3.4; 12.9) | 0.0 | 3 (−1.2; 5.1) | 0.38 | 1.2 (−7.2; 12.2) | 0.31 |
| Eccentric extension 30°/s | 12.6 (−2.3; 19.1) | 0.23 | 10.6 (−1.7; 60) | 0.06 | 8.1 (−12.1; 25) | 0.65 |
| Eccentric extension 90°/s | 12.8 (−9.2; 21.5) | 0.48 | 7 (−4.7; 32.9) | 0.10 | −0.8 (−15.9; 8.3) | 0.91 |
1.4
Discussion
The present study’s main finding was that isokinetic measurement of PT in hip flexion/extension movements displays good to very good reproducibility. The reproducibility was less good for hip Ext during low velocity concentric movement on the right side and low velocity eccentric movement on the left side. This finding may be due to the unilateral nature of our data which differs from most of the reproducibility studies in the literature that average the measurements from the left and right sides. Averaging the values for the two legs before calculating the reproducibility may mask poorer results for one of the two hips. Hence, by studying the reproducibility of each of the two hips separately, we chose the most rigorous method – even though it resulted in lower reproducibility on one side from time to time, as was observed once for the left hip and once for the right. Given our relatively small sample size, a significant variation in the performance of a single subject (due to fatigue or lack of motivation, for example) could have affected the reproducibility for the study population as a whole.
The ICC values in the present study are comparable to those found in the literature . In fact, the concentric FI tests were more reproducible in our study (with ICC > 0.90, versus values of between 0.6 and 0.9 in the literature), whereas there was a trend towards poorer reproducibility for the Ext in concentric tests.
The good reproducibility of the concentric-mode hip FI measurements observed here (ICC > 0.83) contrasts with the moderate reproducibility (ICC < 0.67) reported by Emery et al. . This difference in reproducibility may be explained in part by the latter authors’ test protocol, which required subjects to successively perform eccentric and concentric work with the same muscle group during an extension-flexion movement (i.e. an eccentric extension phase and a concentric flexion phase). This change in contraction mode is difficult for subjects to master and may explain (at least in part) the observed poorer reproducibility.
The ICC values for eccentric tests of the Ext (0.68 < ICC < 0.8) were slightly lower than the values for concentric tests (0.62 < ICC < 0.94); this was probably due to greater compensation through use of all the posterior trunk muscles. Hence, the results for eccentric hip Ext tests must be interpreted with caution. Our data agree with those published by Emery et al. in what is the only literature study (to the best of our knowledge) to have examined the reproducibility of eccentric-mode hip muscle strength measurements. However, Emery et al. did not analyze the same muscle groups (concentric and eccentric hip FI and adductors) as we did here. The authors observed good reproducibility for the adductors but only very moderate reproducibility for the FI.
A Bland and Altman plot showed that in addition to good overall reproducibility, the small differences between W1 and W2 PT values did not result from systematic, major bias. In fact, satisfactory ICC values sometimes mask the presence of significant, systematic bias that could affect the validity of the measurements.
In the present study, we only observed slight fixed bias in our test measurements: the W2 values were almost always greater than the W1 values. This finding may be due to a learning effect for the isokinetic contraction mode, which is very rarely encountered in activities of daily living or during sport. This isokinetic learning effect has already been reported many times in the literature and underlines the importance of performing a warm-up series on the machine in order to prepare the muscle for effort and, above all, enable the subject to learn to perform this type of movement. Using a Bland and Altman plot, Dugailly also observed that the 95% confidence interval was broader for the Ext than for the FI.
Comparison of the PT values for the right and left legs did not reveal significant differences, except for concentric movement of the hip FI at 180°/s in W1. Hence, we did not observe a statistically significant dominance effect for the median hip FI and Ext PT values in this population. In view of the breadth of the 25 th /75 th percentile interval for certain measurements (notably in eccentric mode at low velocities), some of these results may need to be considered with a degree of caution. However, the interval was usually below 10% of the absolute value measured. Our present results are in agreement with other studies on isokinetic hip muscle strength , in which significant differences between the values for the right and left hip Ext or FI were not observed (regardless of the contraction mode or test velocity). However, it is noteworthy that two of these studies (Dugailly and Calmels ) examined subjects performing little or no sporting activity, whereas the two others investigated elite sportspeople performing essentially symmetric sports (sprinting in Alexander and ice hockey in Smith et al. ). In contrast, Tippett reported a dominance effect for the hip’s FI and external rotators in an isokinetic movement study of 16 baseball pitchers. This dominance effect may be due to the specific features of the pitching action: after accurately describing the hip’s rotational and flexion-extension forces for the pitcher’s stance leg and kick leg, Tippett attributed the presence dominance effect to the asymmetric nature of the pitching action.
Hence, as has already been emphasized by Calmels , the values of the contralateral hip can serve as a reference during rehabilitation of an injured hip in a population of sedentary subjects or of people playing symmetric sports. In contrast, it appears that use of the contralateral hip as a reference value is not recommended for high-level sportspeople in asymmetric sports like baseball.
The number of subjects included in the present reproducibility study may appear to be low. Nevertheless, given our use of a protocol with three tests at 7-day intervals (rather than just two tests, as is often the case in the literature) and the estimated precision of the measurements for which we wished to calculate the reproducibility, we were able to calculate a priori that the requisite sample size was 10.
We selected the velocity range (a slow [60°/s] and a rapid [180°/s] concentric-mode test and a single slow, eccentric-mode test) by analogy with isokinetic knee testing – the reproducibility of which has been comprehensively evaluated. Low velocity, concentric tests probe the muscles’ performances in terms of maximum strength, whereas the high velocity concentric tests tend to give more information on “explosive” strength. We limited the high velocity test to 180°/s because preliminary experiments revealed that the subjects had great difficulty performing the movement at higher velocities (notably at 240°/s): the truly isokinetic range of joint movement was very narrow or even inexistent, which reduced the measurements’ reliability. In eccentric-mode knee tests, high velocities do not necessarily provide additional information and are more likely to induce injury than low test velocities. This is why we chose to use only slow velocities for the eccentric hip tests.
Our decision to only test the eccentric strength of the hip Ext was based on two considerations:
- •
eccentric testing of the hip FI would significantly worsen lumbar lordosis;
- •
analysis of the prevalence of muscle damage in sportspeople shows that the hamstrings are most often affected .
Given this context, studying the reproducibility of the eccentric strength of the hip FI muscles was not a priority. Hence, in view of the risk of back injury during eccentric testing of the hip FI and given our research group’s strong focus on studying hamstring injuries, we decided to study the eccentric strength of the hip Ext only.
There is no consensus on the position that the subject should adopt for this type of strength test: as in the present study, some authors have performed these tests with supine subjects and others have preferred the standing position . The position during testing is an important parameter. The lying position is most frequently used in the literature (i.e. in eight of the ten identified studies) and appears to be the most reproducible (by minimizing compensations as much as possible). However, certain authors have emphasized that the standing position is more physiologically relevant. Indeed, it has been shown that there was a better correlation between hip muscle strength and the velocity of movement in the standing position than in the lying position (Farrar and Thorland ).
Hence, we initially opted for hip strength tests in the standing position but finally decided to use the lying position in view of:
- •
the poor reproducibility observed in preliminary tests (difficulty in limiting compensations, due to the angle of the trunk);
- •
the inability to standardize the subject’s position with respect to other studies.
In fact, despite the results reported by Guskiewicz et al. (good test reproducibility, with ICC values between 0.82 and 0.96), we believe that the reproducibility of measurements in the standing position is dependent on too many parameters. We thus deliberately preferred the more reproducible position over the more natural position.
1.5
Conclusion
The present study demonstrates that isokinetic measurement of the concentric and eccentric PT generated by the hip FI and Ext is highly reproducible. We also note that the absence of a significant difference between the muscle groups on the dominant and nondominant sides. This enables the use of isokinetic testing in routine clinical practice by taking the healthy, contralateral limb as a reference (except in very asymmetric sports, such as baseball).
We believe that clinical application of this isokinetic test procedure will be of value in many fields: back problems, post-surgical rehabilitation of the legs and rehabilitation after leg amputation and hamstring muscle injuries.
Related posts:
 Médecine manuelle – ostéopathie en France
Manual medicine – osteopathy in France organization – education – fields of expertise
Médecine manuelle – ostéopathie en France
Manual medicine – osteopathy in France organization – education – fields of expertise
 Neuromuscular and muscle-tendon system adaptations to isotonic and isokinetic eccentric exercise
Neuromuscular and muscle-tendon system adaptations to isotonic and isokinetic eccentric exercise
 Evaluation of a multidisciplinary consultation of diabetic foot
Evaluation of a multidisciplinary consultation of diabetic foot
 European accreditation of programmes of care in physical and rehabilitation medicine. Goals, pilot phase, new procedure
European accreditation of programmes of care in physical and rehabilitation medicine. Goals, pilot phase, new procedure
 Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


