Repeat Operation After Total Knee Arthroplasty
The specific incidence of and causes for repeat operation after total knee arthroplasty (TKA) continue to change with time. In the early experience with hinge and condylar knees, repeat operations were most frequently required for prosthetic loosening, knee instability, and sepsis. Twenty-five years ago, patellofemoral complications accounted for up to 50% of repeat operations.1 With improved prosthetic designs and better surgical technique, repeat operations are becoming less frequent. Polyethylene wear is now the leading cause for reoperation, and prosthetic loosening, instability, and patellofemoral problems are rare.
In this chapter, the incidence and causes of repeat operation after 4500 consecutive posterior cruciate ligament (PCL)-retaining primary TKAs followed for a mean of 15 years are discussed. Among the 4500 knees, 244 required repeat operations. Some causes are obviously prosthesis specific. Nevertheless, my experience gives an overview of the complications most likely to be seen today in an arthroplasty practice.
Femoral Component Loosening
Isolated femoral component loosening has been very rare, regardless of whether the component was cemented or cementless. Failure of either femoral fixation method accounted for approximately 2% of the 244 knees requiring reoperations. The incidence of femoral loosening ran 0.01% per year at a mean of 15 years. The success of a cementless femur depends on the quality of primary fixation at the time of the arthroplasty. A reliable standard is to test the difficulty of extracting the femoral trial as a way to quantify the fit. Both cemented and cementless femurs are vulnerable to late loosening in the presence of severe osteolysis.
Tibial Component Loosening
Isolated cemented tibial component loosening also has been infrequent and accounted for approximately 2% of the 244 knees requiring reoperations. It, too, has an extremely low incidence of 0.01% per year failure at a mean of 15 years. In the presence of severe osteolysis, however, tibial loosening is more prevalent.
Cementless tibial components are more likely to loosen than cemented components, with the incidence depending on their design and the accuracy of implantation. Components fixed with screws or those using metals with high ingrowth potential are more likely to enjoy long-term success.
In this series, cementless tibias were implanted in only 40 knees, or approximately 1% of patients, and never with ancillary screw fixation. Among these 40 knees, four have loosened, for an incidence of 10% at a mean of 25 years of follow-up.
Advocates of cementless tibial fixation prefer and succeed with ancillary screw fixation. However, long-term concerns exist with this technique in regard to potential screw migration, because the tibial tray normally undergoes some long-term subsidence. This movement would allow well-fixed screws to begin to penetrate the undersurface of the polyethylene, and the screw holes in the tray would allow ingress of wear debris to the bone with subsequent osteolysis. Examples of both these complications have been described in the literature.2 Newer trabecular metal cementless tibial components that do not require screw fixation may hold promise for long-term cementless fixation.3
Patellar Complications
Metal-Backed Patella
When tibial components adopted metal backing in the late 1970s and early 1980s, the same rationale was used to metal-back the patella. The metal backing was to add support to the polyethylene and decrease focal forces across the fixation interface. It would also allow for application of a porous surface for bone ingrowth, permitting cementless fixation. In the mid-1980s, failures of metal-backed patellae were reported resulting from accelerated polyethylene wear with early designs.4 In retrospect, it was appreciated that the application of a metal backing diminished the polyethylene thickness to such an extent that accelerated wear would occur, especially if the patella tracked asymmetrically (usually with some lateral tilt). In this series, 9 of the 87 implanted metal-backed patellae failed as a result of wear. None were implanted after 1986. Most surgeons now avoid metal-backed patellae except of the mobile-bearing variety, for which the same high incidence of failure has not been reported.5
All-Polyethylene Patella
Since the mid-1980s a three-pegged all-polyethylene patellar component has become the state of the art. Among the 4241 all-polyethylene patellae in this series, none has been revised for wear or patellar instability. There have been four traumatic fractures. Three were treated conservatively, and one required a patellectomy.
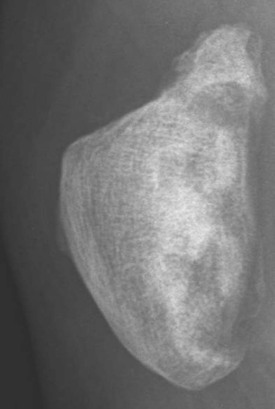
A small number of avulsion fractures were seen that usually involved a few millimeters of the superior pole of the patella (Figure 15-1). Most often, these were incidental findings at routine follow-up. Occasionally, they were symptomatic for approximately 6 weeks, during which time the patients were advised to avoid high forces across the patellofemoral articulation, such as with ascending stairs and rising from a sitting position without arm support.
Six repeat operations were performed for patellar complications. Three involved shearing-off of the three lugs from an early design. The junction between the lug and the patellar component was reinforced, eliminating this complication. The cause of this complication also involved the presence of an abnormal shearing force resulting from imbalance in the quadriceps mechanism. The conformity of the articulation would tend to keep the patella located in the trochlear groove, whereas the soft tissue imbalance would attempt to pull the patella toward the lateral side.
Three other repeat operations involving a cemented three-pegged all-polyethylene patella were for late patellar loosening. One of these patients had undergone a lateral retinacular release, and examination of the patellar bone at repeat operation showed signs of osteonecrosis, possibly contributing to the loosening.
Unresurfaced Patella
Among the 4500 consecutive primary TKAs, 178 patellae were left unresurfaced. Specific indications existed for not resurfacing the patella in this series.6,7 At mean 15-year follow-up, 7 of these patients had required secondary resurfacing between 1 and 15 years after initial arthroplasty. Only 4 of the 6 patients experienced complete relief of their pre-resurfacing pain, emphasizing the point that the unresurfaced patella invites repeat operation, even if it may not be the source of persistent discomfort.
Because the complications of resurfacing with a cemented three-pegged all-polyethylene patella are so rare, many surgeons now consider not resurfacing only young, active, osteoarthritic male patients who fulfill specific selection criteria and only after a careful discussion with them of the pros and cons of not resurfacing. Regional and individual exceptions exist to this viewpoint, in which leaving the patella unresurfaced is common.
Related posts:
 Flexion Contracture Associated with Total Knee Arthroplasty
Flexion Contracture Associated with Total Knee Arthroplasty
 Total Knee Arthroplasty in Rheumatoid Arthritis
Total Knee Arthroplasty in Rheumatoid Arthritis
 Sepsis and Total Knee Arthroplasty
Sepsis and Total Knee Arthroplasty
 Staying Out and Getting Out of Trouble During Total Knee Arthroplasty
Staying Out and Getting Out of Trouble During Total Knee Arthroplasty
 Posterior Cruciate Ligament Retention Versus Substitution
Posterior Cruciate Ligament Retention Versus Substitution
 Total Knee Arthroplasty After Osteotomy
Total Knee Arthroplasty After Osteotomy



