Release of Simple Syndactyly
Donald S. Bae
DEFINITION
Syndactyly refers to the failure of separation between adjacent digits, resulting in “webbed” fingers.
Congenital syndactyly is classified according to the extent of digital involvement and the character of the conjoined tissue.
Complete syndactyly extends to the digital tips (FIG 1A), whereas incomplete syndactyly ends proximal to the fingertips (FIG 1B).
Simple syndactyly refers to digits connected only by skin and soft tissue. Complex syndactyly denotes bony fusions between adjacent phalanges.
Complicated syndactyly refers to the interposition of accessory phalanges or abnormal bones between digits.
ANATOMY
Understanding of normal digital web space anatomy guides surgical reconstructive efforts.
Typically, the index-long and ring-small finger commissures are U-shaped, whereas the long-ring web is V-shaped.
The nonglabrous skin of the normal web space is sloped about 45 degrees from proximal-dorsal to distal-volar, extending to roughly the midpoint of the proximal phalanx.
The natatory ligaments (or superficial transverse metacarpal ligament) help form the web contour and join adjacent lateral digital sheets.
Normally, each digit is vascularized in part via a radial and an ulnar digital artery, which arise from the bifurcation of the common digital arteries.
In simple syndactyly, adjacent digits are joined by varying amounts of skin and soft tissue.
The nail plates may or may not be fused.
The joints, ligaments, and tendons of the affected digits usually are normal.
It is of critical surgical importance that the bifurcation of the digital arteries and nerves may be abnormally distal in cases of syndactyly.
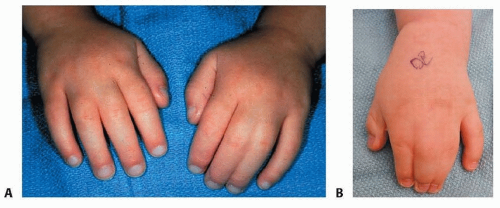 FIG 1 • A. Simple incomplete syndactylies of the bilateral third web spaces, with the left hand more severely affected. B. Simple complete syndactyly of the second and third web spaces is seen in another patient. Observe the conjoined fingernail (synonychia) between the long and ring fingers. (Copyright © 2006 Children’s Orthopaedic Surgery Foundation.) |
PATHOGENESIS
Syndactyly represents a failure of differentiation and is so classified by the embryologic classification of congenital anomalies adopted by the International Federation for Societies for Surgery of the Hand.
Embryologically, the digits arise from condensations of mesoderm within the rudimentary hand paddle of the developing upper limb.
During the fifth and sixth weeks of gestation, interdigital clefts form through the process of apoptosis, or programmed cell death, beginning at the digital tips and proceeding in a distal to proximal direction.
The apical ectodermal ridge regulates this embryologic process, in conjunction with fibroblast growth factors, bone morphogenetic proteins, transforming growth factors, homeobox gene products, and the sonic hedgehog protein.
Interruption of this precise and highly regulated process results in syndactyly.
NATURAL HISTORY
There is no potential for spontaneous resolution.
Given the importance of independent digit function in today’s world, surgical release is recommended for simple complete syndactyly, with few exceptions.
When digits of differing lengths are joined, the syndactyly may lead to deformity and growth disturbance, with the longer digit typically developing a flexion contracture and angular deviation toward the shorter digit.
Simple complete syndactyly of the long-ring interspace may be well tolerated and may not significantly compromise growth or function in young patients.
Simple incomplete syndactylies may be aesthetically subtle and cause little functional compromise. In these situations, observation may be considered.
PATIENT HISTORY AND PHYSICAL FINDINGS
The diagnosis of syndactyly usually is not subtle, and the extent of digital involvement typically is readily apparent.
Syndactyly is the most common congenital hand anomaly, with an estimated incidence of 1 in 2000 to 2500 live births.
The true incidence of syndactyly is unknown, in part because of the difficulty distinguishing mild simple syndactylies from normal web spaces.
The third web space is most commonly affected (50%), followed by the fourth (30%), second (15%), and first (5%) web spaces.
Males tend to be more commonly affected than females and whites more than blacks or Asians.
Inheritance is thought to be autosomal dominant with incomplete penetrance and variable expression.
The absence of differential motion of the affected digits suggests a complex or complicated syndactyly.
Because the joints and tendons usually are normal, patients typically have flexion and extension creases over the interphalangeal joints and active digital motion.
Syndactyly may exist in isolation or may be seen in the context of associated clinical syndromes, including Poland syndrome, Apert syndrome, and constriction band syndrome. For this reason, careful evaluation of the entire upper extremity, contralateral upper limb, chest, and feet is advised.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs of the affected digits or hand are routinely obtained to accurately classify the syndactyly and assess for bony fusions or interposed or accessory bones (FIG 2).
Magnetic resonance imaging (MRI), angiography, or other diagnostic studies are not typically obtained because they do not assist surgical decision making or operative treatment.
NONOPERATIVE MANAGEMENT
Nonoperative management may be considered for mild, simple incomplete syndactyly.
Nonoperative treatment also may be favored in cases of complicated syndactyly with the so-called “superdigit” or in cases of complex polysyndactyly because of the difficulty in achieving reproducible functional improvement with surgical release.
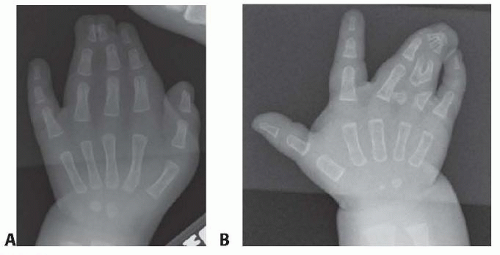
FIG 2 • A. Anteroposterior (AP) radiograph of the patient depicted in FIG 1B. Note the simple complete syndactyly between the index and long fingers and a complex complete syndactyly between the long and ring fingers. B. AP radiograph depicting a complicated polysyndactyly in another patient.
However, given the importance of independent digital motion—particularly in the current keyboard-driven digital age—nonoperative treatment of simple complete syndactyly is not recommended.
SURGICAL MANAGEMENT
General surgical principles include the following:
Digits of differing lengths should be released early to prevent deformity and growth disturbance of the affected digits.
Digits should be operated upon on only one side at the same time to avoid vascular embarrassment.
Local skin flaps should be used to recreate the commissure to avoid scar contracture and “web creep.”
Zigzag lateral flaps should be created to avoid longitudinal scar contracture.
Judicious defatting of the skin flaps should be performed to facilitate skin closure, reduce tension across the flaps, and improve the aesthetics of the reconstructed fingers.
Preoperative Planning
The timing of surgery must be considered in preoperative planning.
There is great variability in recommendations of when releases should be performed.
Flatt8 wrote, “I believe one should ask not how soon the operation can be done but rather how late the functional demands of the hand will allow postponement of surgery.”
In general, releases are performed between 6 and 24 months of age.
As mentioned, digits of differing lengths (eg, thumb-index syndactyly) should be released earlier to avoid secondary deformity.
Positioning
The patient is positioned supine with the affected limb supported on a hand table.
Placement of a sterile or nonsterile tourniquet must be sufficiently proximal to allow access to the antecubital fossa, if full-thickness skin graft is to be taken from that site.
If the skin graft is to be harvested from the inguinal region, the ipsilateral groin is prepared and draped to allow for easy access.
Before draping, a surgical pen may be used to mark the inguinal skin fold when the hip is flexed; graft harvest along this axis will allow for a more aesthetic skin closure.
Care should be taken to harvest the skin graft lateral to the femoral artery to avoid transfer of hair-bearing skin.
Approach
The principles of separation for simple complete syndactyly are well accepted; however, there is tremendous variation in the surgical incisions and skin flap designs used for these operations.
All use local tissue to reconstruct the interdigital commissure, and all employ interdigitating zigzag lateral flaps. Dorsal skin flaps are preferred for commissure reconstruction because of their pliability and ability to recreate the normal dorsal-proximal to volar-distal slope of the web.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



