Fig. 5.1
Mechanism in compression-extension causing Colles’ fractures
Traumas in compression-flexion, rarer, causing a palmar displacement. For example, the Goyrand-Smith fracture, where there’s a palmar displacement of the inferior extremity of the radius (Fig. 5.1′).
Fig. 5.1′
Mechanism in compression-flexion causing Goyrand-Smith’s fracture
Associated injuries are frequent and related to the inclination [2] and prono-supination during the trauma:
In radial inclination/supination, the associated injuries are generally a fracture of the scaphoid or a sprain of the scapholunate ligament.
In ulnar inclination/pronation, the associated injuries are generally injuries of the triangular complex, the ulnar styloid process (Gérard-Marchand fracture), or the lunotriquetral ligament (Fig. 5.2).
Fig. 5.2
Associated injuries are frequent and related to the inclination and prono-supination during the trauma
In practice, fractures in old patients with osteoporosis will produce metaphyseal fractures without associated injuries, while fractures in young patients are often caused by more violent traumas and are frequently complex with associated injuries.
This kind of fracture can modify the radioulnar index with an injury of the triangular complex and/or another radioulnar lock, disturbing the dynamics and/or stability of the radioulnar frame (see Chap. 2).
In this chapter, we will only see the injuries of the inferior extremity of the radius that don’t lead to these complications.
5.2 Clinical and Paraclinical Signs [3]
A radiological assessment must be realized after any trauma causing pain or wrist deformity (Fig. 5.3).

Fig. 5.3
Fracture of the radius with posterior tilt and associated injury of the ulnar styloid process
It’s very rare to find a normal X-ray in case of a fracture of the radius, displaced or not.
We always check the radial pulse and the absence of injury of the median nerve. This verification can require a quick reduction of the fracture, or even emergency surgery.
If there’s a doubt and pain persists, we immobilize during 15 days before realizing another clinical (palpation of the radial metaphysis, triangular complex, and anatomical snuffbox) and paraclinical (scintigraphy, scanner, MRI) exploration.
5.3 Therapeutic Process and Surgical Treatment [4–7]
Several classifications of the wrist fractures are proposed. They mainly depend on the position of the fracture line, the distal fragment’s direction of displacement, and the fracture’s complexity (comminuted fracture). These classifications guide the orthopedic and surgical treatment [6].
The orthopedic treatment is used in stable and non-displaced fractures of the distal radius. It always starts with a palmar immobilization of the forearm in order to immobilize the flexion/extension and the prono-supination.
On the other hand, surgery is used in displaced fractures of the metaphysis or joint surface, and that are instable after reduction [8].
The surgery aims to obtain an anatomical restitution of the joint surface and relative length of the 2 bones, to respect the forearm frame. They guarantee quality functional recovery.
5.3.1 Reduction
It’s always realized with an external maneuver at first, with the help of an image intensifier.
We also take shots in traction to analyze better the fracture lines.
In joint fractures [8], arthroscopy can be interesting to check the quality of reduction.
If the fracture is stable, this reduction can be enough. For example, displaced fractures of the radial metaphysis in children are usually stable once reduced and don’t require complementary surgical fixation.
Generally, in adults, fractures are unstable once reduced and require osteosynthesis in most cases.
There’s an exception for fractures of very osteoporotic bones in old patients, to which no osteosynthesis will give enough stability. In these rare cases, the reduction is followed by a palmar immobilization of the forearm, without osteosynthesis.
If we obtain the reduction with the external maneuver, we can do the reduction with closed surgery.
If we don’t do the reduction with the external maneuver, the fixation has to be realized with open surgery.
5.3.2 Fixation (Fig. 5.3′)
Fig. 5.3′
Osteosynthesis with pins or plate
The goal is to obtain a stable fixation allowing the consolidation without secondary displacement, ideally with an early mobilization of the wrist.
There are three ways to realize the osteosynthesis: the pins are generally put percutaneously and can only be dorsal or lateral. In fact, there’s a major risk of injury for the noble palmar elements (radial artery and median nerve).
Screwed plates are more stable than pins, and this stability is all the more important since the screws can have an angular stability inside the plate (locked screws).
It would be more logical to place these elements on the side of the displacement to oppose it: dorsal pins for fractures with dorsal tilt and palmar plate for fractures with palmar tilt [9].
However, complications are frequent with plates placed on the dorsal radial side. In particular, there are many ruptures of the extensor tendons (extensor pollicis longus) that are very vulnerable when contacting with the osteosynthesis plate. These complications have made many surgical teams abandon this technique.
A third way to do it is putting and external fixator.
The principle is to use the ligamentotaxis induced by the wrist distraction. The problems of this technique are the high number of CRPS related to distraction and the inaccessibility of the posteromedial fragment of the radius on which no ligament is inserted.
To prevent these complications, it’s recommended to realize a distraction as little as possible and to place at least one posteromedial pin combined with the external fixator.
5.4 Rehabilitation and Orthotic Treatment [4, 6, 10–12]
These fractures have the false reputation of being “benign,” but they can cause important losses of strength and mobility that can have functional aftereffects [13].
5.4.1 Rehabilitation Protocol (Fig. 5.4) [14, 15]
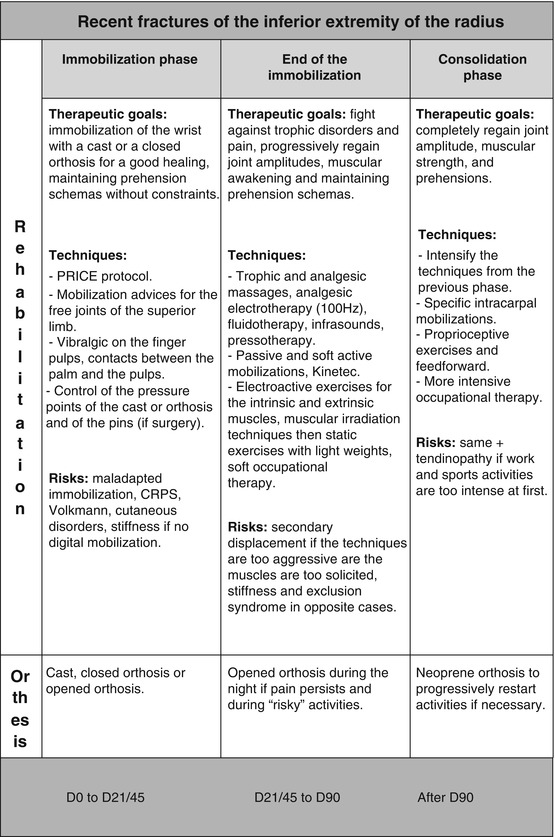
Fig. 5.4
Rehabilitation protocol
This protocol can follow the surgery or orthopedic treatment and can be modified depending on the healing evolution.
This evolution is regularly controlled with X-rays.
The protocol has many common points with the one for the fractures of the scaphoid; therefore, we won’t describe here the techniques used in both pathologies.
In practice, the protocol is often more progressive as these injuries mainly occur in old people. Trophic disorders, pain, and stiffness are then often longer and more important.
From a symptomatic point of view, the patients often describe pain on the ulnar side of the wrist that can have various causes:
Increase of the radial slope leading to overwork of the ulnar stabilizers
Injury of the triangular complex
Changes in the radioulnar index with a “long” ulna that increases the ulno-carpal constraints
The consequences of these unbalances for the therapist are:
Predominant reinforcement of the ulnar stabilizers in case of increased radial slope (Figs. 5.5 and 5.5′)
Fig. 5.5
The increase of the radial slope favors the carpal gliding towards the ulna, which increases the constraints at this level
Fig. 5.5′
In this case, the therapist must intensify reinforcement techniques for the ulnar stabilizers to oppose this phenomenon
Predominant reinforcement of the pronator quadratus in injuries of the triangular complex (Figs. 5.6 and 5.6′)
Fig. 5.6
An injury of the triangular complex can cause pain and instability if it’s associated with an injury of one of the two other radioulnar locks
Fig. 5.6′
Reinforcing the pronator quadratus participates in limiting pain and instability (combined with the other radioulnar “key” muscles) (see Chap. 2)
Exercises in ulnar decoaptation in case of long ulna (Figs. 5.7 and 5.7′)