Radionucleotide Imaging and Pet Scanning of the Hip
Sandip Basu
Abass Alavi
Introduction
The functional radionuclide imaging modalities can subserve a valuable adjunct to the clinical and radiologic assessment of hip abnormalities, especially when employed and interpreted judiciously. The abnormalities where the modalities (Table 24.1) can play a role are (a) assessment of painful hip arthroplasties (to differentiate between aseptic loosening and periprosthetic infection), (b) transient osteoporosis of the hip, (c) aseptic/avascular osteonecrosis, (d) Legg–Calvé–Perthes disease, (e) early arthritis of the hip joint, and (f) stress fractures of the femoral neck or of the pubic rami. A number of nuclear medicine procedures have been used in the aforementioned disorders (Table 24.2).
Bone Scan (Synonym—Skeletal Scintigraphy)
Traditionally, skeletal scintigraphy with 99mTc-methylene diphosphonate (MDP) had been utilized to study and make pathophysiologic and etiologic diagnosis of these entities in conjunction with other modalities and clinical information. The tracer adheres to bone by chemical absorption, referred to as chemisorption onto surface of bone trabeculae, especially to the newly forming amorphous bone (onto the phosphorous groups of calcium hydroxyapatite).
Table 24.1 Entities Where Radionuclide Imaging Modalities Have Been Investigated for Potential Utility | |
|---|---|
|
Gallium Scan and Indium-111 Leukocyte Imaging
Both gallium scan and 111In-white blood cell (WBC) imaging are particularly helpful in differentiating infection such as osteomyelitis from other differential diagnosis, for example, aseptic loosening. 67Ga scintigrams are interpreted together with 99mTc-labeled bone scintigrams: For diagnosis of osteomyelitis or infection, the defined criteria followed are the distribution of activity on both studies is spatially congruent and the relative intensity of gallium activity is greater than that of 99mTc-MDP activity or the distribution of activity on both studies is spatially incongruent, with gallium activity exceeding bone activity. The study is negative for infection if gallium scintigraphy is negative or the relative intensity of gallium activity is less than that of bone activity, in case both studies demonstrate congruent distribution tracer activity. In the radiolabeled WBC scans WBCs from the patient are tagged with the radioisotope, for example, 111In, and then injected back intravenously into the patient. The tagged leukocytes subsequently localize to areas of relatively new infection.
Table 24.2 Radionuclide Imaging Techniques Employed in Skeletal Disorders | |
|---|---|
|
FDG-PET/CT Imaging
18F-Fluoride PET/CT Imaging
Though analogous to bone scan, this modality has substantially superior resolution compared to planar scanning and is being investigated for its superiority in various skeletal disorders. The molecular principle for 18F-fluoride PET is that it is, in contrast to bone imaging phosphonates, directly incorporated into the bone matrix, converting hydroxyapatite to fluorapatite. As the tracer is not protein bound, imaging can be done faster (1 hour after injection). Compared to traditional bone scans (which takes around 4 hours) this study could be completed by around 90 minutes overall.
Bone Marrow Imaging with Planar and Pet Imaging
Noninvasive imaging for assessing the functional activity of the bone marrow has primarily involved 99mTc-labeled tracers, such as 99mTc-sulfur colloid and 99mTc-nanocolloid. The other tracers in this domain are 111In-chloride and radiolabeled WBCs. Bone marrow imaging has been primarily employed in hematologic and oncologic settings (3,4,5,6,7). As they represent affection of hip as a part of a generalized disease and do not specifically belong to hip joint abnormalities, they were considered beyond the purview of this chapter. Three separate compartments can be evaluated (the reticuloendothelial system, the erythroid compartment, and the myeloid compartment) with appropriate tracers. Recently, with the development of PET tracers using 18F-FDG and 18F-FLT, cellular metabolism and proliferative activity can be studied. This methodology offers the advantages of superior resolution and better quantification.
Table 24.3 The Various Stages of Avascular Necrosis, Clinical Symptoms, Pathophysiologic Aspects, and the Skeletal Scintigraphic Findings in These Stages | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Aseptic Osteonecrosis of Hip (Synonym—Avascular Necrosis/Ischemic Necrosis)
Salient Points on the Disease Pathophysiology
Osteonecrosis of the femoral head involving the hip joint could be traumatic (the most common form) and atraumatic in origin. The reason for atraumatic osteonecrosis is poorly understood and includes certain risk factors: (i) High-dose corticosteroid use, (ii) excessive alcohol intake, (iii) sickle cell anemia, (iv) Gaucher disease, (v) systemic lupus erythematosus, (vi) coagulopathies, (vii) hyperlipidemia, (viii) organ transplantation, (ix) caisson disease, and (x) thyroid disorders. The annual incidence in the United States is approximately 10,000 to 20,000 new cases. Around 50% of patients with atraumatic hip osteonecrosis are estimated to be bilateral and frequently may involve multiple bones in the body like the shoulder, knee, and talus, although it most commonly affects the femoral epiphysis. The basic pathogenesis is impaired blood supply to the bone, but it is not always clear what causes that impairment. To highlight the vascular compromise as an important factor, the terms “avascular necrosis (AVN)”/“ischemic necrosis” are often used synonymously. The common pathway for the pathogenesis is that with the bone death of the femoral head, resorption of the dead tissue occurs followed by repair process by new but weaker osseous tissue ultimately leads to subchondral fracture and collapse.
Where can Radionuclide Imaging Help?
The role of skeletal scintigraphy has been stressed as it can aid in detection earlier than plain radiography. Among the various factors guiding the management, stage of the disease is an important determinant and the treatment approaches
vary significantly between early and late phases of the disease. Reduced weight bearing and core decompression is most useful in the earliest stages of the disease. However, one requires remembering the nonspecificity of bone scan which could be positive in trauma, synovitis, and infections and thus the diagnosis should be inferred in conjunction with other clinical and imaging information. Bone scan complements MRI information and these two modalities encompass the noninvasive imaging approach of choice in a high-risk population.
vary significantly between early and late phases of the disease. Reduced weight bearing and core decompression is most useful in the earliest stages of the disease. However, one requires remembering the nonspecificity of bone scan which could be positive in trauma, synovitis, and infections and thus the diagnosis should be inferred in conjunction with other clinical and imaging information. Bone scan complements MRI information and these two modalities encompass the noninvasive imaging approach of choice in a high-risk population.
Bone Scan Findings according to Stages
The bone scan findings in the five stages of AVN are described in Table 24.3.
Salient Features and Temporal Sequence of Bone Scan Findings
Photon-deficient area on bone scan is usually observed around 7 to 10 days after the ischemic insult. This is followed by increased uptake (caused by revascularization and repair) that occurs weeks to months later (Figs. 24.1 and 24.2). The doughnut sign (central photopenia with surrounding zone of increased uptake) represents reactive bone around the infarcted zone, which is seen in the interim period (Fig. 24.3). The decreased uptake in the perfusion and static phases, which is noted soon after early ischemic event is very specific of AVN. False-negative bone scan findings can be seen in (i) bilateral disease (demonstrating bilateral symmetrical uptake) and (ii) at the transition from infarction to revascularization (falsely normal in 6% to 10% of patients) whereas a false-positive scintigraphic pattern can be seen in two ways: (i) Pathologies causing reduced uptake (infection, plasma cell myeloma, osteolytic skeletal metastasis, hemangioma, radiation therapy, etc.) and (ii) pathologies causing enhanced uptake (transient osteoporosis of the hip, arthritis, sympathetic dystrophy, malignancy, infection, hemangioma, stress fractures, etc.).
 Figure 24.1. Bone scan of a patient with avascular necrosis of the femoral head shows increased uptake in the superolateral aspect of the right femoral head, indicative of avascular necrosis but providing little information concerning the structural integrity of the hip. (Images reprinted with permission from Medscape Reference (http://emedicine.medscape.com/), 2013, available at: http://emedicine.medscape.com/article/386808-overview.) |
 Figure 24.2. Planar bone scan of the pelvis in a patient with bilateral avascular necrosis of the femoral head shows marked increased uptake of radiopharmaceutical agent in both hips. (Images reprinted with permission from Medscape Reference (http://emedicine.medscape.com/), 2013, available at: http://emedicine.medscape.com/article/386808-overview.) |
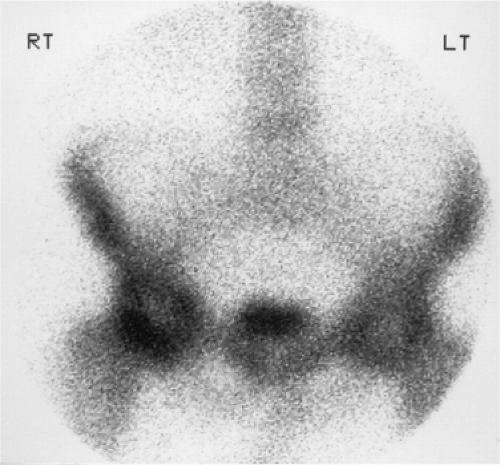 Figure 24.3. Radionuclide bone scan of the pelvis in a 68-year-old man with hip pain demonstrates a bilateral central area of diminished uptake surrounded by a zone of increased uptake in the femoral head consistent with avascular necrosis. (Images reprinted with permission from Medscape Reference (http://emedicine.medscape.com/), 2013, available at: http://emedicine.medscape.com/article/387545-overview.) |
Comparison of Skeletal Scintigraphy, Plain Radiography, and MRI in Diagnosing AVN
Scintigraphy is sensitive and useful in early-stage disease (especially Stage I disease) over plain radiography. Greater sensitivity is observed for MRI compared to scintigraphy by various investigators, with most investigators reporting a sensitivity of nearing 100% for MRI and that for scintigraphy between 81% and 90% (8,9,10), though specificities reported are higher for bone scintigraphy. It is to be noted that bone scintigraphy with a pinhole collimator has greater sensitivity than that of parallel hole collimator even with high resolution.
Research Domains
The recent data from a solitary report indicates that 18F-fluoride PET scan may show early involvement in the acetabulum that is not discernible by other radiographic modalities. In a study by Dasa et al. (11), 9 of 17 hips (8 patients) demonstrated increased acetabular uptake when imaged with 18F-fluoride PET scans that were not seen on MRI, SPECT, or planar bone scan. These data suggest earlier acetabular changes in osteonecrosis may exist that traditional imaging modalities do not reveal. The implications of this finding for patient management is yet unknown.
Assessment of Painful Hip Arthroplasties (to Differentiate between Aseptic Loosening and Periprosthetic Infection)
Pathophysiology
Hip arthroplasty is one of the most commonly performed orthopedic procedures primarily undertaken to treat joint failure caused by osteoarthritis (OA). However, evaluation and treatment of the painful hip arthroplasty is a challenging task.
Table 24.4 Patient Characteristics and Imaging Methods Used by Different Research Groups in Investigating PET in Arthroplasty-associated Infection | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|









