Key Points
- 1.
Radiographs are essential for evaluation and treatment of distal radius fractures.
- 2.
Complete radiographic assessment requires proper technique and all projections necessary to fully evaluate the injury.
- 3.
Interpretation of distal radius fracture radiographs requires more than simple identification of radial inclination, volar tilt, and radial length; routine assessment of several other essential landmarks and parameters is needed to avoid missed pathology and unrecognized malreduction.
- 4.
Radiographs of distal radius fractures provides important information that helps identify the injury mechanism, type, and direction of principle instability, and pattern and components of peri-articular fragmentation.
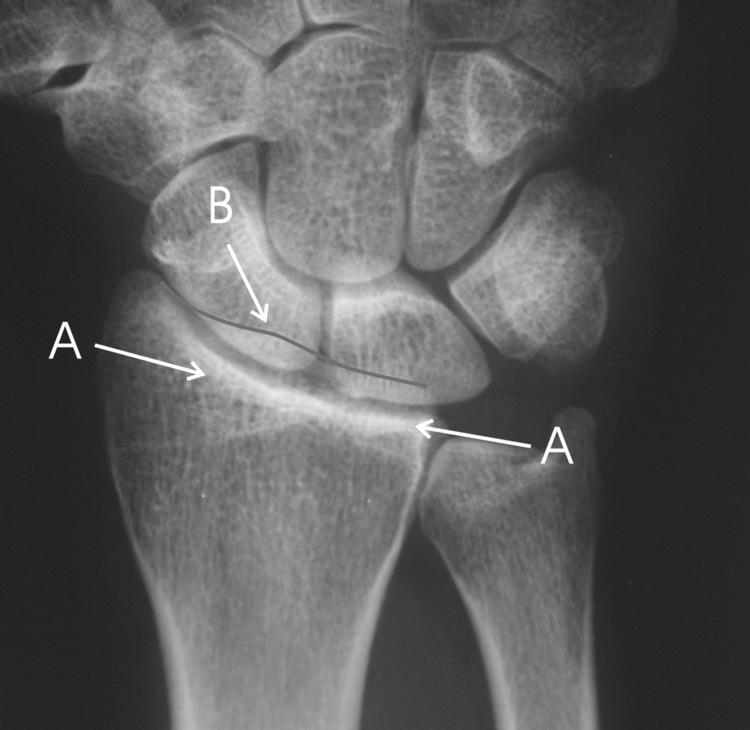
A 60 year-old, right-handed female seamstress/artist fell on her outstretched left arm. She was treated in a splint and now complains that anytime she loads her wrist in dorsiflexion she experiences intense pain. Radiographs show dorsal angulation of the distal fragment and her examination shows moderate deformity with limited forearm rotation ( Fig. 1 ). Other than the dorsal angulation of the distal fragment, what other significant abnormalities require correction in order to alleviate her symptoms?

Importance of the Problem
Of all the joints in the human body, there are none as complex as the wrist. The wrist coordinates synchronous movement of 10 independent bones, allowing rotational motion along all three cardinal axes as well as providing gliding motion in the coronal and sagittal plane. Fractures of the distal radius are the most common fractures of the wrist and represent 17% of all fractures. Although adjunctive modalities such as CT and MRI are certainly helpful in providing detailed information about the morphology of distal radius fractures at a single point in time, there is no question that plain radiographic studies remain the workhorse for the evaluation of wrist injuries, especially at the initial presentation, during operative treatment, and with the routine assessments that are necessary for follow-up care.
The teardrop is best visualized on the 10 degrees lateral radiograph, but can also be identified on the standard lateral radiograph. It represents the outline of the cortical and subchondral bone surfaces of the volar rim of the lunate facet, and is important in maintenance of the sagittal position of the carpus.
The teardrop angle (defined as the angle between the central axis of the radial shaft and the central axis of the teardrop) in normal wrist is 70 ± 10 degrees.
Axial instability patterns of the volar rim can be recognized by depression of the teardrop angle below 45 degrees along with pathologic dorsal subluxation of the central rotational axis of the base of the capitate. Stable reduction includes correction of the dorsiflexed position along with restoration of carpal alignment to a line extended from the volar shaft of the radius.
Volar instability patterns of the volar rim typically present with a normal teardrop angle, but show palmar displacement and shortening of the volar rim. Stable reduction of this pattern of instability should include restoration of length to the volar rim as well as palmar support of the volar fragment.
Interpretation of standard radiographs requires more than simple assessment of radial inclination, volar tilt, and radial length. For instance, the teardrop angle of the volar rim of the lunate facet, loss of congruency of the radii of curvature of adjacent articulating surfaces, identification of the position and displacement of the carpal facet horizon, assessment of the lateral carpal alignment, AP distance, pathologic widening of the distal radioulunar joint (DRUJ), coronal fragment shift, and carpal malalignment are examples of some of the other landmarks and parameters used to identify pathologic conditions that otherwise can be overlooked ( Figs. 2 and 3 ).

The importance of these additional landmarks and parameters has only been recognized relatively recently. Because of this, large numbers of studies in the literature omit recognition of these important radiographic features and should be interpreted with caution as conclusions may be based on incomplete information.
Fernandez and Jupiter characterized distal radius fractures according to the mechanism of injury: (1) bending, (2) shear, (3) axial load, (4) carpal avulsions, and (5) high energy. The character and personality of injuries in each of these groups varies considerably, and it is probably not reasonable to lump these different fracture mechanisms together when evaluating clinical results related to a specific parameter or treatment. Moreover, the expectations and demands in a low demand patient population are considerably different from those in a very active patient population. For this reason, additional caution should be exercised when reaching conclusion from clinical evaluations that are based on clinical data based on a nonuniform population.
Main Question
What is the significance of the features of radiographic assessment in the management of distal radius fractures?
Current Opinion
There is an overwhelming consensus of opinion that radiographs are necessary as part of the evaluation and management of distal radius fractures, and the AO classification is the established standard in the literature for identifying the various types of injury. Despite this, there are differences of opinion on our ability to consistently recognize radiographic pathology and the relative significance of specific abnormalities to clinical outcomes.
Finding the Evidence
- •
Cochrane search: distal radius lateral carpal alignment; distal radius teardrop; distal radius radiographs; distal radius DTV.
- •
Pubmed (Medline): (“distal radius”) AND (“radiograph”) AND (“teardrop” OR “alignment” OR “parameters”).
- •
Articles not in English were excluded from review.
Level I:
Randomized controlled trials: 4
Level II:
Randomized controlled trials with methodological limitations: 5
Level IV:
Case series: 14
Lever V:
Expert opinion: 1
Findings
Three level-one studies examined radiographic criteria in cadaveric specimens and volunteers. One study evaluated the ability of an anatomic tilt view to assess screw penetration in the radiocarpal and distal radioulnar joints in 24 cadavers; this view showed high levels of specificity (0.93) and sensitivity (0.98) of articular screw penetration ( Fig. 4 ). Another study reviewed anthropomorphic variability between left and right specimens with 3D CT scans; no significant difference in radial height, radial inclination, or volar tilt was noted. Another study evaluated the effect of rotational position of the forearm specifically on the dorsal tangential view (DTV) for determining alignment of the distal radioulnar joint. Four transhumeral specimens were used and observers correctly identified abnormalities of DRUJ position as reduced, volarly malreduced, or dorsally malreduced on 94% of the DTV images (97%, 95%, and 92% in the neutral, supinated, and pronated forearm positions, respectively) with high intraobserver and interobserver reliability.





