55 Radial Shortening
Indications
Symptomatic Kienböck disease without lunate collapse (stages 0, I, or II) in a wrist with a positive ulnar variance
Technique
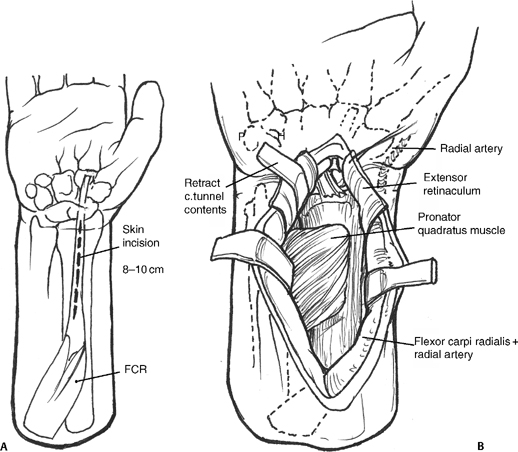
- Palmar incision over the flexor carpi radialis (FCR) tendon beginning at wrist crease and extending 8 to 10 cm up the forearm
- Open FCR tendon sheath and retract tendon in ulnar direction. Incise the floor of the tendon sheath.
- Identify and incise the pronator quadratus (PQ) along its radial margin and elevate from the distal radius (Fig. 55-1A,B).
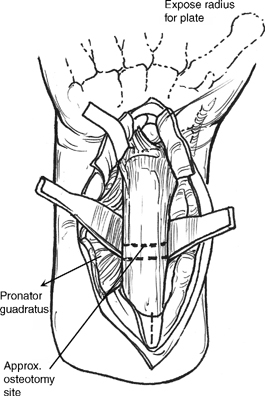
- Place retractors on both sides of the radius. Expose enough of the radius to accommodate a six-hole dynamic compression plate (DCP) (Fig. 55-2). This exposure may require partial elevation of flexor pollicis longus (FPL) origin.
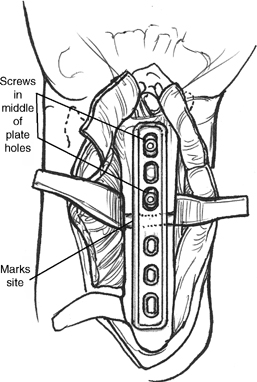
- Apply the six-hole DCP along distal radius. The distal aspect of the plate may have to be bent to match the palmar slope of the distal radius.
- Mark the osteotomy site between third and fourth holes in the plate. Place bicortical screws distal to the planned site of the osteotomy.
Figure 55-1
Figure 55-2
Pearl
The osteotomy should be performed in the metaphysis to increase the chance and rate of healing.
- Remove the screws and plate. Elevate the periosteum at osteotomy site.
- Make the first cut two thirds of the way through the radius. This cut can be either transverse or oblique to the long axis of the radius. A second cut is made parallel to the first, 2 to 4 mm proximal to the initial osteotomy. Complete the first cut and remove wafer of radius.
- Reapply the plate and distal screws. Compress the osteotomy by manual pressure until bone ends approximate. Hold with reduction clamp applied between the proximal plate and radius (Fig. 55-3).
- Secure the proximal portion of the plate using one or two compression screws to compress the osteotomy site. Place the remaining screws in neutral compression (Fig. 55-4).
- Check the alignment of the osteotomized radius and the plate and screw position with fluoroscopy (Fig. 55-5).
 Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
Intra-articular Fractures of the Distal Radius Treated with Dorsal Plate
 Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
Resect Ulnar Styloid Fracture with Repair of Triangular Fibrocartilage Complex
 Sauve-Kapandji Procedure
Sauve-Kapandji Procedure
 Darrach Procedure (Distal Ulna Resection)
Darrach Procedure (Distal Ulna Resection)
 Scaphocapitate Fusion with Lunate Excision
Scaphocapitate Fusion with Lunate Excision
 Capitate Shortening with Capitohamate Fusion
Capitate Shortening with Capitohamate Fusion



