Radial Dysplasia Reconstruction
Carley Vuillermin
Marybeth Ezaki
Scott N. Oishi
DEFINITION
Radial dysplasia represents a spectrum of longitudinal deficiency in radial growth.
This deficiency can be mild or severe based on the deficiency in the radius.
ANATOMY
The anatomic relations of the radial aspect of the wrist are altered due to the variable absence of the radius.
The higher the degree of radial dysplasia, the more divergent from normal anatomic relationships the findings will be. This is critically important when undertaking surgical intervention.
Table 1 Bayne and Klug Classification of Radial Dysplasia
Type
Radiograph
Description
I

Short distal radius; distal epiphysis present, delayed; mild radial deviation
II

Defective growth proximal-distal epiphyses; radius in miniature
III

Partial absence of radius; wrist unsupported
IV

Total absence of radius
Adapted from Bayne CG, Klug MS. Long-term review of the surgical treatment of radial deficiencies. J Hand Surg Am 1987;12(2):169-179.
A consistent but highly abnormal brachiocarpalis muscle has been described in thrombocytopenia-absent radius (TAR) syndrome.14 This muscle spans from just distal to the deltoid insertion directly into the radial side of the carpus and inserts as a broad aponeurotic fan into the carpus, joint capsule, and tendons of the radial wrist.
Many patients have associated thumb hypoplasia.10
Several authors have proposed alterations to this classification in order to better describe the spectrum of presentation. James et al12 added N and 0 categories. N represents patients with a normal radius and carpus but hypoplastic thumb and 0 for patients with carpal abnormalities and
normal radial length. Goldfarb et al9 proposed a type V for more proximal deficiencies.
PATHOGENESIS
Radial dysplasia develops during the period of embryogenesis. During this period, other organ systems are developing and may also be affected, as discussed later in this chapter.
NATURAL HISTORY
The natural history of patients with radial dysplasia clearly depends on the type of dysplasia present and the associated conditions.
Patients with isolated type I or II radial dysplasia usually do not require surgical intervention to address the wrist and radial deformity.
Patients with more severe dysplasia can frequently benefit from surgical intervention.
Many times radial dysplasia is part of a syndrome, and the associated sequelae clearly affect these patients more than the underlying radial dysplasia. The most common associations are with Holt-Oram syndrome, TAR syndrome, Fanconi anemia, and VACTERL (vertebral anomalies, anal atresia, cardiovascular anomalies, tracheoesophageal fistula, esophageal atresia, renal or radial anomalies, limb anomalies).10, 11
An association with several craniofacial syndromes has been well documented.8
PATIENT HISTORY AND PHYSICAL FINDINGS
The most significant finding is radial deviation at the wrist (FIG 1).
If the patient is older, the affected forearm will also be short.
Assessment of adjacent joints is essential. Frequently, there will be associated thumb hypoplasia or absence, and in more severe cases (especially Holt-Oram syndrome), the other digits may be stiff. Elbow range of motion is important and the ability to bring the hand to the mouth once the wrist is in a corrected position should be assessed. Radioulnar synostosis is also sometimes present especially in children with Holt-Oram syndrome.
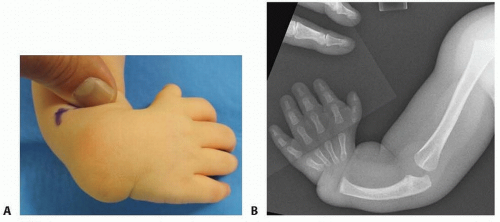
FIG 1 • A. Preoperative photo showing radial deviation of the wrist. B. Anteroposterior (AP) radiograph of the same child demonstrating type IV radial deficiency.
Because of its frequent association with systemic conditions, all patients require careful examination of their spine and cardiac, renal, and hematologic systems.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs should be taken of both forearms to assess stage of radial dysplasia (see Table 1).
In addition, all patients warrant a workup for syndromes and associated conditions, such as Holt-Oram syndrome, Fanconi anemia, TAR syndrome, and VACTERL.
This may require echocardiogram, renal ultrasound, hematologic studies (complete blood count [CBC] and chromosomal fragility studies), and spinal evaluation.
Each treating physician should consider these associations and not assume they have already been worked up, especially if surgical care of the limb is contemplated.
NONOPERATIVE MANAGEMENT
All patients warrant stretching and splinting before consideration of any surgical intervention.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








