Proximal and Distal First Metatarsal Osteotomies for Hallux Valgus
Patient Selection
Indications
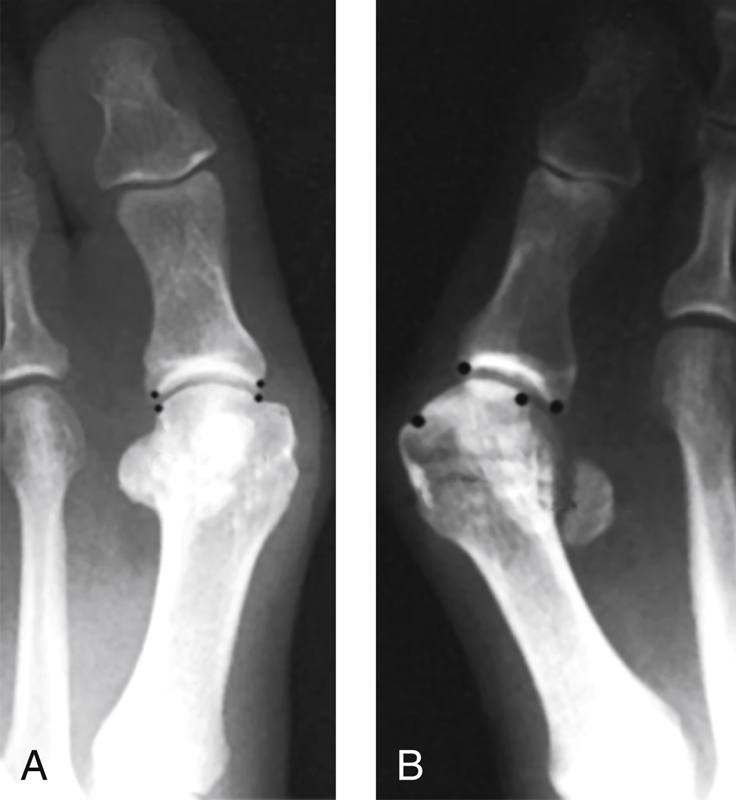
Figure 1AP radiographs show a congruent (A) and an incongruent (B) first metatarsophalangeal joint.
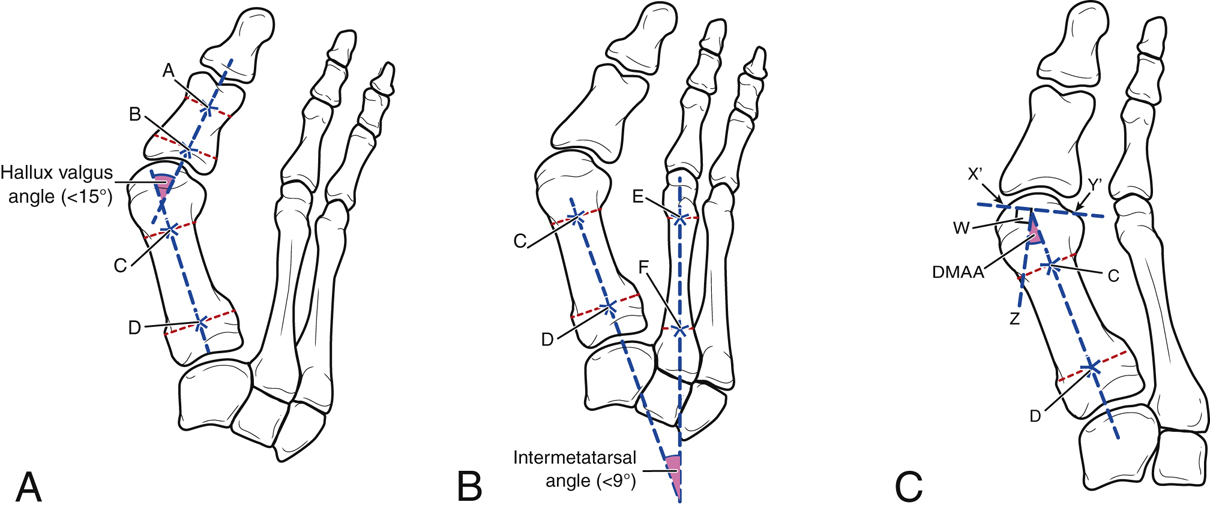
Figure 2Illustrations show measurements that are made on preoperative radiographs to plan surgery for hallux valgus. A, Measuring the hallux valgus angle. A normal hallux valgus angle is less than 15°. A line (A) is drawn down the axis of the proximal phalanx and another line (B) is drawn down the axis of the first metatarsal. C and D are reference points midway between the medial and lateral cortex, at a point 1 cm from the end of the bone. B, Measuring the first-second intermetatarsal angle. A normal first-second intermetatarsal angle is less than 9°. E and F are reference points midway between the medial and lateral cortex, at a point 1 cm from the end of the bone. C, Measuring the distal metatarsal articular angle (DMAA). A normal DMAA is less than 6°. Line C–D delineates the longitudinal axis of the first metatarsal. X′ and Y′ are reference points of the medial and lateral edge of the articular surface. Line W–Z is drawn perpendicular to the line drawn between X′ and Y′. The DMAA is the angle subtended by lines W–Z and C–D.
Clinically symptomatic moderate to severe hallux valgus deformity with congruent first metatarsophalangeal (MTP) joint (Figure 1)
Uncommon; only 2% to 9% of hallux deformities are congruent
Radiographic findings—First-second intermetatarsal angle greater than 13°, distal metatarsal articular angle (DMAA) greater than 15° (Figure 2)
Recurrent hallux valgus more common if congruent joint made incongruent
Triple osteotomies may be indicated for recurrent hallux valgus, hallux valgus interphalangeal deformity, or significant rotational deformity
Juvenile hallux valgus frequently recurs, likely because of underappreciation of the original deformity
Contraindications
Cosmetic concerns
Arthritis of the first MTP joint
Severe metatarsus adductus
Spasticity
Vascular insufficiency
Infection
Severe traumatic soft-tissue concerns
Contracture of first metatarsal phalangeal joint
Preoperative Imaging
Weight-bearing AP, lateral, oblique views of foot centered over tarsometatarsal joint
Measure hallux valgus angle, first-second intermetatarsal angle, DMAA, first MTP joint congruency
Procedure
Room Setup/Patient Positioning
Supine position on standard table
Bump under ipsilateral hip
Mini C-arm on surgical side
Tourniquet
Special Instruments/Equipment/Implants
Crescentic oscillating saw blade
Straight oscillating saw blade
3.5-mm solid small-fragment screw set
0.062-in Kirschner wires (K-wires)
Proximal first metatarsal plate
Surgical Technique
Distal Metatarsal Osteotomy
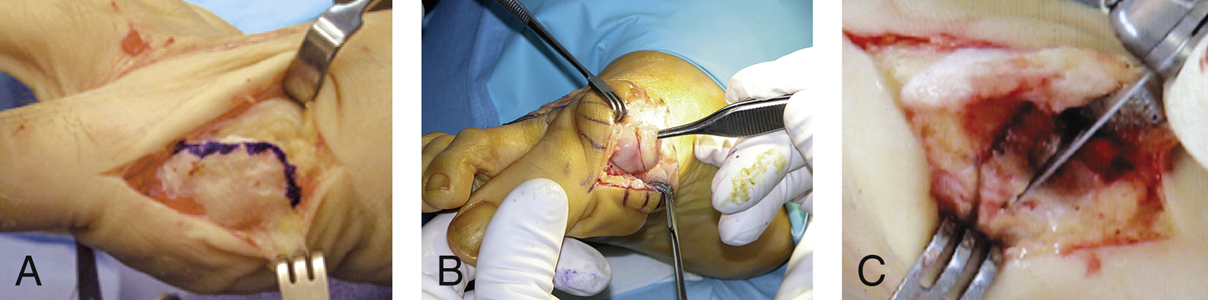
Figure 3Intraoperative photographs demonstrate distal metatarsal osteotomy. A, The medial first metatarsophalangeal joint is shown with the capsulotomy outlined. B, The medial eminence of the cartilage of the first metatarsal head is resected. C, The medial wedge of bone is resected.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


