Providing social services to the older client
James Siberski
Introduction
Today’s older adults are confronted with numerous challenges as they age (Lemme, 2006). The onslaught of baby boomers will change how one ages. In addition to normal age-related changes and the still undefined boomer changes, frequently there are disease states that must also be addressed in order to age successfully. The social service provider plays an important role in assisting older adults to adjust to age-related changes through adaptive changes and devices, and adjust to the disease state through the rehabilitative process.
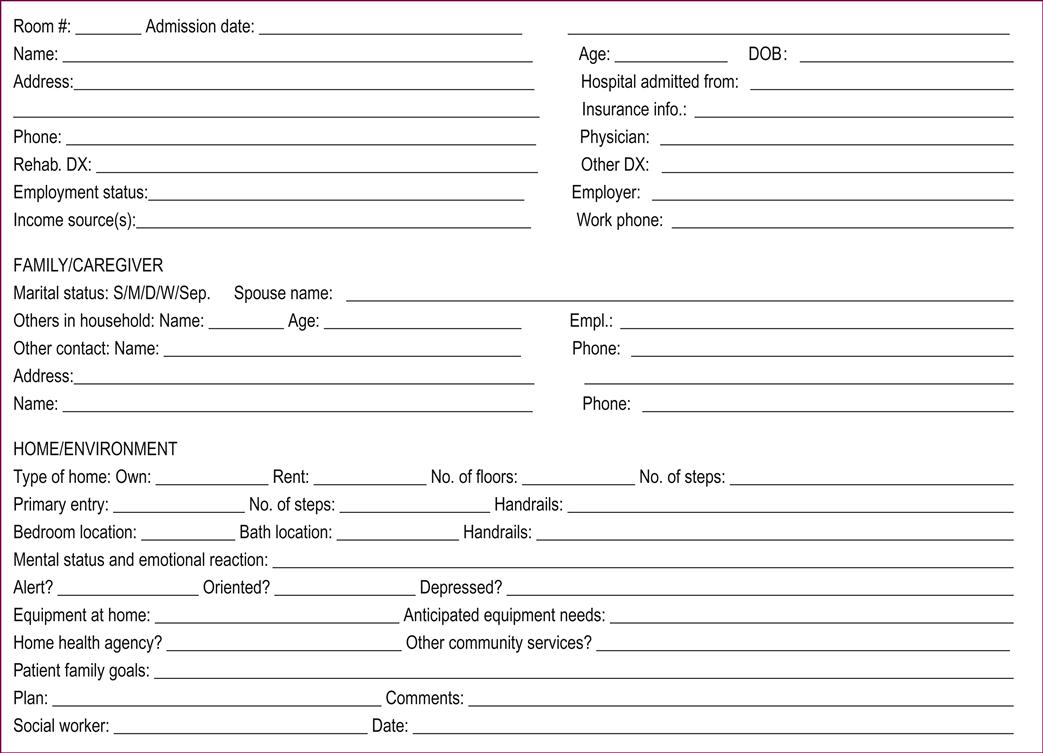
As a member of the rehabilitative team, the social service provider performs a key role. In order to succeed, the team needs specific information from the social worker or geriatric care manager. Initially, this individual completes a comprehensive social work assessment and social history providing important data that will be incorporated into the rehabilitative care plan and enable the older client to achieve his or her goals. While various forms are available (see Form 84.1) for completing this task, in many settings the format is dictated by the agency or department. As a result of education and training, professional social service providers are efficient at completing an assessment, taking a social history, determining needs and strengths, and developing discipline-specific goals. In assessing the elderly, additional considerations must be entertained in order to facilitate the return of the older client to an appropriate placement at the completion of rehabilitation.
Additional considerations in assessment
Additional considerations, which include baby boomers, goal incongruence, cure verses care, client and family perceptions, personality, activities and diversity issues, can either assist or detract from the success of the rehabilitative process.
Baby boomers
All 78 million boomers have experienced every stage of life in their own way; if there was a mold, they broke it, and there is no reason to believe that their older years will be any different (Frey, 2010). Complicating the situation is the diversity of the boomers – Catholics, Jews, Protestants, etc. and African Americans, Native Americans, Hispanic Americans, etc. Social service workers should be aware that they will soon be faced with tremendous diversity and with demands from boomers for services that previously did not exist. Consider their need for social connectivity, i.e. the internet, including its availability in senior living/nursing facilities; social differences, i.e. taste in music and clothing preferences; sex, i.e. different expectations for sexual freedom in nursing facilities; waking and dining time preferences; and support groups for their emotional wants (Feldman, 2012), all of which will place additional stress on the social service provider. It will be necessary for social histories to be specific for: past and current drug use; sexual preferences; desirable leisure activities; and how that boomer views rehabilitation. This will create an interesting challenge for the social service provider in goal incongruence, cure vs. care, client and family perceptions, personality, activities and diversity issues.
Goal incongruence
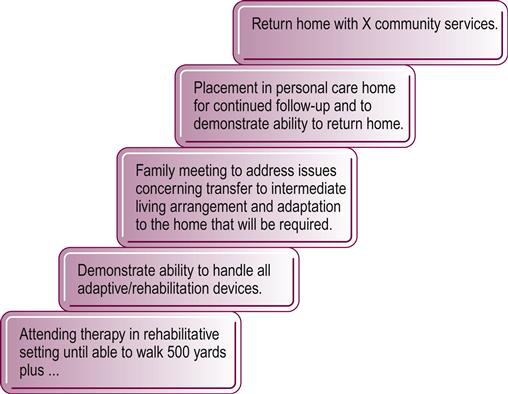
In the rehabilitative process, the team often determines that the appropriate placement is a structured living arrangement while the older client believes that the appropriate living arrangement is their home. This goal incongruence between team and client is not restricted to just placement but can include driving, employment, financial management and other issues of autonomy. Unresolved goal incongruence hinders the rehabilitative process. In addressing this issue, the social worker should capitalize on the client’s motivation to go home by communicating that several steps are necessary for attaining this goal. By graphically demonstrating the intervening steps toward the goal (see Fig. 84.1), the social worker utilizes the client’s motivation to achieve the rehabilitative team’s goal as well as his or her own personal goal. In Figure 84.1, several possible steps are identified in a rehabilitation process to capitalize on a patient’s motivation to return to their own home. Step one is attending therapy until X% of function is gained. Step two is learning to use adaptive devices. Step three is discussing the required supports and home adaptations with the social worker and family. Step four is placement in a personal care home for a period of 6 months in order to demonstrate the ability to do X. Step five is to return home. While returning home may not even be an attainable goal, the social worker should avoid making this an issue so as not to detract from the rehabilitative process.
Cure vs. care
The social service assessment should address the older client’s desire for care or for cure. The rehabilitative team needs to be aware that older clients need care. Care is the opportunity for such things as intimate touch by the physical therapist, occupational therapist, nurse or physician. Care also gives purpose to the day. The older client needs to go to the outpatient clinic on Monday; to cardiac rehabilitation on Tuesday; to the pharmacy on Wednesday, etc. The older client’s regular interaction with the social worker or home health aide is an opportunity to socialize and to feel valued by the provider. In contrast, cure, by eliminating therapy or treatment, creates a loss. Recognizing this situation, the rehabilitative team can then plan around the loss so that the client will not be excessively concerned.
Client, family and others’ views of rehabilitation
The social service provider needs to assess both the client’s and the family’s view of the expected outcomes of rehabilitation. If the prevailing view is that the rehabilitative plan will not help or that the client is doomed to fail, the client’s potential for success is seriously impaired. The social worker must provide education, appropriate for reading and comprehension level, and perhaps even involve other team members in the education process.
Personality
Knowledge of the client’s personality in their youth is beneficial in determining possible issues and appropriate team approaches prior to therapy (Hoyer & Roodin, 2009). Someone who was guarded at age 40 tends to be more guarded, if not suspicious, as they age, especially when under stress. Since an overly friendly approach would increase suspicion and hinder therapy, the social worker should employ a passive friendly approach. This would entail briefly discussing the rehabilitation process and then pulling back and letting the client ponder the information. Next, could be one or two more short visits by the social worker asking if there are any questions or concerns, followed by gently asking the client what are their thoughts and when might they be ready to start the rehabilitation process? This process can take a bit more time but yield more positive results. If someone had always demanded perfection, and with therapy, could not expect 100% return to function, the social worker would also need to address pertinent limitations.
Activities
An assessment of the older individual’s activities and activity style enables one to get a good understanding of the severity of the client’s condition and its impact on the client’s life. The passionate reader, who after completing therapy has 50% mobility, may be satisfied, whereas the passionate walker would be upset. The social worker needs to address this situation by first discovering the needs met by walking, e.g. stress reduction, and then by providing either alternative methods to meet the needs or by modifying the walking pattern, e.g. a slower pace, a shorter distance, or a different frequency, which might require the involvement of other members of the team. A bright light at the end of the rehabilitation tunnel will motivate the older person to work harder and ultimately experience better results from rehabilitation.
Diversity
Social service providers need to be cognizant of ethnic diversity and cultures. African Americans, Pacific Asian Americans, American Indians and Hispanic Americans all have different belief systems. The older American Indian will approach rehabilitation differently from the African American. The manner in which the team approaches, addresses and instructs the client is important to the outcome of therapy (Quadagno, 2005). The social worker should educate the team as to how to address diverse populations as well as their cultural beliefs in terms of medical care, and in fact, if they are even accepting of traditional medical care.
The geriatric care manager
A Geriatric Care Manager (GCM), as defined by the National Association of Professional Geriatric Care Managers, is a health and human services professional, such as a gerontologist, social worker, counselor or nurse, with a specialized body of knowledge and experience related to aging and elder care issues. The GCM assists older adults and persons with disabilities in attaining their maximum functional potential. They strive to respect the autonomy of the individual and to deliver care coordination and support services with sensitivity, in order to preserve the dignity and the respect of the individual. This includes end of life care and the client’s right to choose his or her wishes for rehabilitation or end of life care. A program spreading across the United States of America is Physician Orders for Life Sustaining Treatment (POLST), which ensures the client’s wishes are communicated and honored as to what kind of medical treatment the client wants toward the end of their life (McDonnell, 2013). Additionally, the GCM is an experienced guide and resource for families of older adults and others with chronic needs. As time progresses and as baby boomers age, the rehabilitative team will work hand in hand with this newly emerging professional. Clinical journals, business publications and weekly news magazines frequently discuss the current concept of care management for older individuals. The GCM can be quite helpful to the social worker in terms of assessment and understanding the older person in need of rehabilitation.
When discharge approaches, the social worker and the rehabilitation team need to consider post-rehabilitation requirements and needs of the client and family. Those requirements and needs include the home, durable medical equipment, home health and community services.
The home
A home visit by members of the rehabilitation team allows family members to be interviewed in a familiar, non-threatening setting. It allows therapists to evaluate for barriers and adaptations that may be needed. Occasionally, a home may be dangerous or inappropriate for a patient’s return. Extreme clutter, filth, lack of utilities, or disrepair may require community intervention. The social worker will have to refer these rare situations to the Protective Service Unit of the Area Agency on Aging or some other appropriate agency. A first-hand view of the home environment helps the social worker prepare the family for the patient’s return and also helps to coordinate community services for the patient’s return home.
Durable medical equipment
Most rehabilitation patients require the use of assistive devices, if only for a short time. Ordering durable medical equipment (DME) in a managed care climate requires knowledge of preferred provider relations and limits of coverage. Patients and families rely on social workers for this knowledge.
Basic items such as canes, walkers and wheelchairs are covered by most insurance carriers for appropriate patients. Larger items such as lifts, continuous passive-motion units and even hospital beds are less readily available and may not be covered at all. Items like lift chairs or stair glides are rarely, if ever, covered by insurance. Some DME suppliers have previously used lift chairs and stair glides, as well as other items available at reduced cost.
Some patients injured under workers’ compensation or automobile plans may be covered for special items. Each individual has to be reviewed separately.
Some rehabilitation facilities or agencies for the disabled may employ an equipment adaptor. This professional person modifies and customizes medical equipment to individual needs. This can be a very helpful service for the geriatric patient.
Home health
Medicare and most major insurance plans cover rehabilitative and nursing services in the home after the patient has been discharged from a facility if a skilled service (a PT or a RN) is ordered by a physician. In some cases, a nurse’s aide may be covered for personal care, such as bathing. As with DME, many carriers are now requiring the use of preferred providers for home health services.
It should be noted that rural areas are often underserved by home health rehabilitative services. This can delay the initiation of care in the home.
Many people are under the impression that Medicare or other insurances provide for private nurses or aides in a patient’s home. Medicare has never covered this service and most other plans have long since discontinued such benefits. There are many agencies that offer this help for a fee.
Community services
The following are useful community services that have traditionally helped older people to remain at home; however, as public funds for these programs have dwindled, agencies have initiated fee-for-service arrangements. This has resulted in shorter waiting lists and faster start-up for services. Of course, it has also resulted in increased costs to the older consumer.
An Area Agency on Aging (AAA) is a local, public agency funded by federal and state monies; the agencies were created to provide support for older people in their homes. Some of the services offered include homemakers, personal care aides, friendly visitors, meals on wheels and so forth. A means test determines eligibility, and the services are generally limited to one or two hours a week. Some AAA offer personal attendant care or Title XX (Lamp II or Options) programs designed to help the most physically challenged individuals stay at home. Agencies on Aging are generally run by county governments. Phone numbers and addresses can be found in the blue pages of the telephone book or on the internet.
Chore services may be available through AAA or another public agency. This useful program can help to build ramps, attach handrails, or provide other minor adaptations. All materials are purchased by the individual receiving the service. Contact the AAA for more information.
Perhaps the best known service is meals on wheels (MOW), which provides a full meal for the homebound individual on 5 days a week or more. There is generally a fee charged for this service.
Adequate transportation services are the most common need of the elderly, especially for the geriatric rehabilitation patient. Most communities offer some type of subsidized transportation for eligible individuals. These programs function as a cross between a bus and a taxi. The vehicles, usually modified vans, travel specified routes but require advance notification of appointments. Vans equipped with wheelchair lifts are available, but extra notice may have to be given. Ambulance transport for routine medical appointments is rarely covered by insurance and is very expensive. Many ambulance providers offer a wheelchair van service at more reasonable rates.
Placement
Despite the best efforts and the fervent hopes of all, the goal of returning home may not be possible for all patients. Inadequate progress in therapy or insufficient support at home may make nursing home placement the only appropriate course of action. The social worker has to be sensitive to feelings of guilt, abandonment and hopelessness as he or she guides the patient and family through the application process. Furthermore, if the realities of modern healthcare make the first choice of a facility unachievable, the social worker must be frank and straightforward in dealing with placement issues. At all times, lines of communication must be kept open to make the patient’s transition as smooth as possible.
Conclusion
While the social assessment and history provide a good basis for the rehabilitative process, it is important to be cognizant of the older person’s special needs. Assessing and evaluating these additional considerations enhances the social worker or social service provider’s opportunity for positive outcomes from the rehabilitative effort. The social worker’s counseling skills, knowledge of community resources and ability to provide education throughout the rehabilitation process helps the client and family cope with the process and reach their rehabilitation goals. Social workers need to pay close attention to the research and developments surrounding the baby boomers in terms of rehabilitation expectations. This information will develop in the near future and should be sought out by social service providers as it is made available.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


