Fig. 2.1
This image demonstrates the five main phases of throwing: wind up, cocking, acceleration, deceleration, and follow-through. The stride phase is part of the lower body kinetic chain [Reprinted from DiGiovine NM, Jobe FW, Pink M, Perry J. An electromyographic analysis of the upper extremity in pitching. Journal of Shoulder and Elbow Surgery. 1992 1(1): 15–25, with permission from Elsevier]
The Kinetic Chain
The kinetic chain is defined as the coordinated sequence of body movements that generate force to perform a particular action. In the throwing athlete, the kinetic chain starts when force is generated from the ground and is transmitted to the legs, the hips, torso, and the shoulder. Finally, the arm acts as the delivery mechanism of that energy [1, 4]. Coordinated movements transmit energy in a manner greater than what the individual joints could develop on their own. Using more body segments within the kinetic chain can create a greater maximum velocity to the overhead throw [5]. The goal of the athlete’s kinetic chain is to develop the optimal force while applying minimal joint loads during movement [6]. When deviations in ideal body mechanics occur, individual joint loads may change with distal segments overcompensating. As a result, the athlete is prone to overuse and to injury. For example, approximately 50 % of patients with superior labral anterior posterior (SLAP) tears have signs of core weakness and deficits in hip flexibility and hip abductor and extensor strength [7–9]. The clinician should evaluate the entire kinetic chain when evaluating the at risk painful shoulder.
Evaluating the entire kinetic chain in a complex movement, like throwing, is challenging [10]. Studying individual parts of the kinetic chain in isolation, however, can provide greater understanding when put in the context of the entire kinetic chain. Coordination of the entire kinetic chain is critical to proper positioning of the arm during throwing. Sufficient power of the lower torso is essential to generate ball velocity [11]. Core and lower extremity weakness creates an unstable platform for the thrower. In fact, weakness in the gluteal region, torso, and scapular region has been postulated to contribute to injury in throwing athletes.
Other areas to be inspected include lead leg internal hip rotation, lead leg quad tightness, and ankle range of motion. All “weak links” in the chain will lead to “downstream difficulties .” The clinician must evaluate the entire kinetic chain to determine weak points that place the overhead throwing athlete at risk. Prompt care to address these abnormalities through muscle training, stretching, and improved throwing mechanics is necessary to prevent kinetic chain abnormalities that could result in shoulder injury [12].
Shoulder Mechanics
The elite overhead athlete can produce shoulder internal rotation velocity of 7000° per second. This is the fastest recorded motion by a human [1, 2]. This maximum velocity is achieved when the athlete externally rotates the arm to the maximal point of external rotation or the “set point.” Seasoned athletes can obtain >130° of hyper-external rotation during the late cocking phase of throwing (Fig. 2.2). To achieve this amount of external rotation, adaptive changes in the glenohumeral mechanics are necessary. In abduction and external rotation, the inferior humeral articular surface rotates putting the anteroinferior shoulder capsule on tension. During the follow-through phase, the distraction force on the shoulder approaches 750 N or about 80 % of the pitcher’s body weight [1, 4, 13]. As a result, the posterior capsular tissue hypertrophies and tightens to adapt to these high distraction forces in order to help decelerate the arm. Over time, tightness in the posterior capsule shifts the center of rotation more posterosuperior on the glenoid so that the greater tuberosity does not impinge on the posterior glenoid (Fig. 2.3). The altered center of rotation relieves tension off the anteroinferior capsule resulting in a functional “pseudolaxity ” of the anterior shoulder [12]. Pseudolaxity in the anterior shoulder can also be a result of a disruption in the labral ring surrounding the glenoid. If the labrum becomes detached posteriorly, the humerus can displace to this detached area due to the loss of labral restraint. This results in pseudolaxity on the opposite (anterior) side of the detachment.
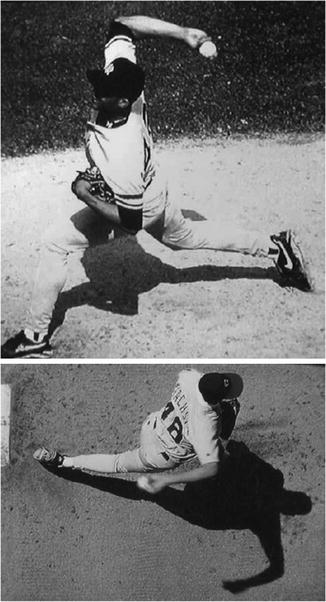
Fig. 2.2
This image demonstrates a baseball pitcher at the point of maximal external rotation or “set point” during a pitch. Notice the position of the legs and torso as elements of the kinetic chain [Reprinted from Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology part I: pathoanatomy and biomechanics. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2003; 19(4): 404–420, with permission from Elsevier]
Fig. 2.3
(a) Normal orientation of the glenohumeral joint leads to rotator cuff impingement. (b) With tightening of the posterior inferior glenohumeral ligament, the humeral head moves posterior-superior and results in loss of the anterior capsule tension and a decreased cam impingement of the greater tuberosity on the posterior glenoid. This results in an anterior pseudolaxity. (c) Demonstrates the superimposed humeral head positions [Reprinted from Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology part I: pathoanatomy and biomechanics. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2003; 19(4): 404–420, with permission from Elsevier]
The cocking phase of the throwing motion is separated into an early stage and late stage. During the early stage, the deltoid muscle is activated and begins to place the arm and hand in the throwing position. During late cocking, the supraspinatus, infraspinatus, and teres minor are all activated to place the arm in abduction and external rotation. At this time the lower body begins shifting forward. This allows energy from the ground to be transferred through the athlete’s kinetic chain resulting in a greater end force at the throwing hand [1, 2]. At the end of the late cocking phase, the shoulder reaches the “set point” [10, 12].
During the early acceleration phase , the triceps, pectoralis major, latissimus dorsi, and serratus anterior fire to maximize the energy in the kinetic chain. The deceleration phase has a high torque point as all muscles eccentrically contract to slow down the arm motion [1]. At this point, the center of gravity has shifted over the forwardly planted foot channeling the energy of the kinetic chain in the lower body. Finally, in the follow-through phase, the body rebalances forward motion, while the muscles return to a resting state.
Pathomechanics of Labral and Rotator Cuff Injury
Throwers with shoulder injury commonly describe the feeling of a “dead arm.” A “dead arm ” is any pathologic shoulder condition in which the thrower is unable to throw with preinjury velocity and control because of a combination of pain and subjective unease in the shoulder [7, 12]. The throwing arm is prone to injury because it requires greater abduction and external rotation to perform athletic activities compared to a non-throwing arm. Several authors have hypothesized that this greater range of motion is a result of “micro-trauma ” or “micro-instability ” to the anterior capsule [14]. Halbrecht studied the biomechanics of the shoulder and determined that anterior instability is not part of the pathology in the dead arm [15]. Other studies have similarly demonstrated that labral lesions are more commonly associated with dead arm syndrome instead of micro-trauma or micro-instability [12, 16].
Andrews is credited with first describing superior labral injuries. Snyder et al. further characterized SLAP injuries [17, 18]. Type II SLAP tears are defined as superior labral and biceps anchor detachment from the supraglenoid tubercle. Type II SLAP tears are common in throwing athletes, particularly tears involving the posterosuperior region (Fig. 2.4) [19]. Type II SLAP repairs comprise approximately 10 % of all shoulder procedures and are the second most common shoulder arthroscopic surgery [20, 21]. The pathomechanics of labral injury are a complex interplay between activity demands and anatomy [12]. O’Brien described the inferior glenohumeral ligament (IGHL) as a two cable system [22]. Usually, the anterior and posterior cables support the humeral head like a sling while in abduction; however, if the posterior cable becomes contracted, from hypertrophy related to repetitive throwing, it can shorten and push the humeral head superiorly [23]. The hypertrophied tight posteroinferior capsule is the initial insult that shifts the humeral head allowing for hyper-external rotation, perceived pseudolaxity, and greater ease obtaining the set point. This improved throwing mechanism is not without consequences. During the throwing motion, hyper-external rotation leads to abnormal impingement and abrasion damage to the rotator cuff [16]. The hyper-external rotation changes the vector force of the biceps tendon to a more vertical and posterior direction during abduction and external rotation [7, 12]. This vector and subsequent biceps muscle contraction create a torsional force across the posterior-superior labrum (Fig. 2.5). Abnormal twisting through the biceps origin on the glenoid leads to torsional overload and shear force injury to the labrum and rotator cuff fibers [16]. The labrum is eventually detached from its anchor as a result of this posterior-superior shift and hyper-external rotation: a “peel-back” phenomenon results.

Fig. 2.4
Arthroscopic image demonstrating labral detachment from the glenoid. This disruption can allow for humeral displacement resulting in pseudolaxity on the opposite region of the glenoid
Fig. 2.5
The position of maximal external rotation results in a vector change for the biceps tendon. During overhead movement, the altered vector creates a peel-back mechanism as the biceps pulls on the labral complex [Reprinted from Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology part I: pathoanatomy and biomechanics. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2003; 19(4): 404–420, with permission from Elsevier]
Although Andrews et al. proposed that superior labral injuries are the result of longitudinal pull on the biceps anchor during the deceleration of the arm, others have proposed that hyper-twisting may be the mechanism causing labral injury [8, 12]. Kuhn performed a biomechanical study that supported the hyper-twisting in the acceleration phase as the mechanism recreating a labral injury [24]. This implies the biceps and superior labrum complex is “peeled off” instead of “pulled” from bone in the deceleration phase [12].
Approximately, one third of all patients with SLAP tears also have rotator cuff tears [20]. Given this association, Walch and Jobe described internal impingement as abduction and external rotation inducing a pinched posterosuperior rotator cuff between the glenoid labrum and greater tuberosity of the humerus [14, 25]. Impingement in this area may also explain the partial articular-sided rotator cuff tears commonly seen in throwing athletes. Morgan et al. reviewed arthroscopic exams and found that rotator cuff tears were also found in 31 % of throwers being treated for SLAP lesions [19]. Of these tears, 38 % were full thickness tears located in the midportion of the rotator crescent, and 62 % were partial-thickness cuff tears in labral lesion-specific anatomic locations. The superior subluxation of the humerus combined with repetitive torsional loading from hyper-external rotation has been postulated as the cause for location-specific partial-thickness cuff tears [12]. The combination of labral pathology and rotator cuff tears is a complicated multifactorial process that ultimately results in loss of shoulder function and/or athletic performance.
Related posts:
 Evaluation of Bone Loss and the Glenoid Track
Indications and Techniques for Double-Row Fixation
Adhesive Capsulitis: Diagnosis, Etiology, and Treatment Strategies
Retracted Subscapularis Tears
Throwing Acquired Anterior Rotator Interval Pathology
Distal Suprascapular Nerve Compression: Spinoglenoid Ligament Release
Evaluation of Bone Loss and the Glenoid Track
Indications and Techniques for Double-Row Fixation
Adhesive Capsulitis: Diagnosis, Etiology, and Treatment Strategies
Retracted Subscapularis Tears
Throwing Acquired Anterior Rotator Interval Pathology
Distal Suprascapular Nerve Compression: Spinoglenoid Ligament Release
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


