CHAPTER 5 Preparatory practice for the yoga art of breathing
 āyāma, the yoga art of breathing
āyāma, the yoga art of breathing  ads, Yoga-Sūtras, and Ha
ads, Yoga-Sūtras, and Ha ha-Yoga-Pradīpikā, breathing is described as the essential process related to life.
ha-Yoga-Pradīpikā, breathing is described as the essential process related to life.Basic anatomy and physiology of respiration
External and internal respiration
Respiration consists of two processes: external and internal respiration. External respiration consists of all processes involved in the intake of oxygen and the elimination of carbon dioxide through the lungs. Internal or cellular respiration is the absorption of oxygen, metabolic processes that produce energy, and the elimination of carbon dioxide through the body cells. This acts to regenerate the cells. External respiration also serves other functions, such as smelling and producing sounds such as speaking and singing, laughing, and coughing (Hauke 1980).
The passage of air
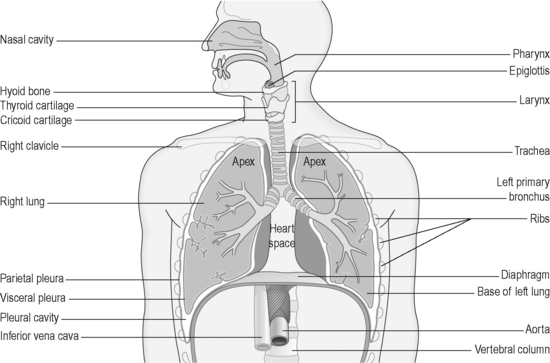
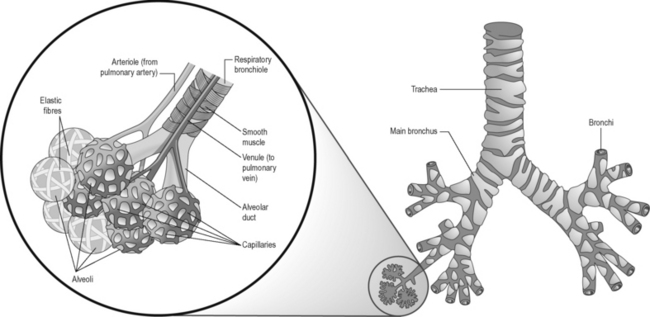
Air enters the system through first the nostrils, then the nasal cavity and the paranasal sinuses. After this comes the pharynx, which consists of three parts: (1) the upper pharynx, behind the nose and connected to the ears via the eustachian tube; (2) the middle pharynx, where food and respiratory pathways cross; and (3) the lower part, connecting to the larynx (Figure 5.1). The structures from the nostrils to the lower pharynx form the upper respiratory system, whereas the larynx is the beginning of the lower respiratory system. The epiglottis covers the larynx during swallowing, interrupting the passage of air. The larynx produces the voice and also the cough reflex to protect the lower structures – the trachea, bronchi, bronchioli, and alveoli of the lungs. The lungs contain about 300 million alveoli, surrounded by pulmonary capillaries (Figure 5.2). Oxygen and carbon dioxide are exchanged between the alveoli and the pulmonary capillaries by diffusion through the respiratory membrane.
The muscles of respiration
The muscles of inspiration
The main muscles of inspiration are the diaphragm and the external intercostal muscles. Parts of the internal intercostal muscles are also involved (Netter 2006).
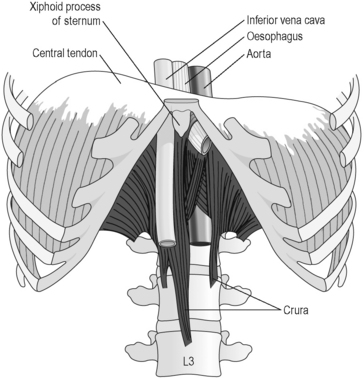
The diaphragm is a dome-shaped, musculotendinous structure, separating the thoracic from the abdominal cavity (Figure 5.3). It is attached to the upper three lumbar vertebral bodies via the crurae, which are tendinous pillars. It is also attached to psoas and quadratus lumborum muscles through the arcuate ligaments, the lower six ribs and their cartilages, and the xiphoid process of the sternum. Good diaphragmatic function assists other structures, and vice versa.
The thoracic cage
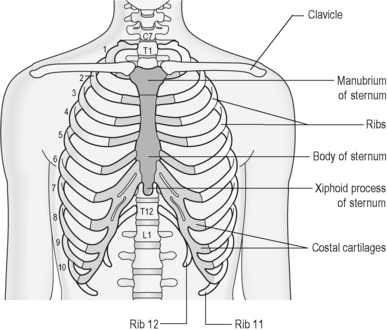
The thoracic vertebrae, the ribs, and the sternum form the thoracic cage, the skeleton of the chest (Figure 5.4). This protects the thoracic organs; the respiratory muscles are also attached to the thoracic cage.
The ribs and their movements with inhalation and exhalation
There are 12 pairs of ribs. The upper seven ribs, the true ribs, are directly connected to the sternum by separate costal cartilages. The eighth to twelfth ribs are the false ribs. The costal cartilages of the eighth, ninth, and tenth ribs are fused, forming the costal arch and connected to the costal cartilage of the seventh rib. Ribs 11 and 12, the floating ribs, are connected just to the thoracic vertebrae, but not the sternum. All other ribs are also connected to the thoracic vertebrae. The costovertebral joints are between the head of the rib, the vertebral body, and the intervertebral disc. The costotransverse joint is between the costal tubercle and the tip of the transverse process. The many different joint planes throughout the different segments of the thoracic spine and the corresponding ribs lead to rib movements in different planes around different axes and therefore to a very complex movement pattern of the ribs during inhalation and exhalation. The three main movement directions can be summarized as follows: (1) elevation of the lower ribs increases the transverse diameter of the thorax; (2) elevation of the upper ribs increases the anteroposterior diameter of the thorax and raises it; (3) elevation of the middle ribs increases both diameters. Ribs 11 and 12 move like callipers to create more space in the lower thorax (Kapandji 2008).
The spine
The thoracic spine bends backwards slightly. B K S Iyengar (2009) gives an elegant description that the ninth thoracic vertebra and the sternum move slightly towards the chin. As a result the physiological curves of the spine become flatter (Hartman 2001). Good mobility of the costovertebral joints is important for breathing. Good mobility of this area also improves the blood supply and drainage of the sympathetic chain that is close to the costovertebral joints.
The sternum
During inhalation the sternum moves forwards and upwards. Anterior movement of the upper sternum is more than that of the lower sternum (Kapandji 2008). This also involves various movements of the costal cartilages, the sternocostal joints, and the costochondral junction and is important for rib movement. In connection with sternal mobility the transverse thoracic muscle is particularly relevant and should be stretched and mobilized.
The rhythm and volume of respiration
There is a significant difference between the normal respiratory volume of 500 ml and the maximum capacity of respiration of up to 5 litres (Martini & Nath 2008). In quiet breathing the main respiratory muscles are used for inhalation; exhalation is passive, by elastic rebound. The emphasis can either be on the contraction of the diaphragm or on raising the ribs through contraction of the external intercostal muscles to increase thoracic volume so that air can be drawn into the lungs. Normally diaphragmatic breathing is deeper – 75% of total volume – whereas costal breathing is shallower – 25% of total volume. It can be further differentiated between high, clavicular breathing, intercostal mid breathing, and diaphragmatic breathing (Iyengar 2009). In full breathing in yoga all areas can be integrated. Capacity is greatest if the ribs are raised when the diaphragm is pulled down. In forced breathing the accessory muscles of inhalation and exhalation are used. In general, quiet deep breathing moves more air than forced, noisy breathing. The normal respiratory rate is 12–18 breaths per minute, slightly higher in children. It is directed by the breathing center in the medulla oblongata, influenced by the concentration of oxygen and carbon dioxide in the blood, the autonomous nervous system, and emotions. It is also adapted to movement (Hauke 1980).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


