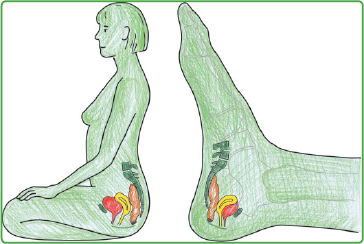
22 Pregnancy and Birth Midwives and specialists from associated professions are able to integrate a great deal of practical and background information from reflexotherapy of the feet (RTF) into their work. This includes the care given to the pregnant woman from the time after conception to the care of the mother and baby in the postpartum period. Although pregnancy is a normal biological process, an increasing number of women suffer from a multitude of complaints during this special time. Basically, we adhere to the rule that RTF support in pregnancy, during and after the birth, is experienced as extremely pleasant and stabilizing by the pregnant woman, even if she does not have any immediate complaints. At the beginning we advise regular care via the feet (roughly once a week) from the fourth month of pregnancy onward. Frequently though, we observe that natural life processes nowadays are complicated by all kinds of irritations and increasing difficulties, and it is obvious that pregnant women often need help. It should be noted that for the most part the dosage of individual therapeutic grips for pregnant women is only half the usual dosage, at least at the beginning, until the personal threshold for the grips offered has been experienced. Usually we make a first assessment as part of the normal care, in particular when the pregnant woman contacts the midwife at an early stage in the pregnancy. Then RFT can be a treasured accompanying measure throughout the following months. However, if there is little remaining time until the birth, situations involving brief and acute treatment often occur. Under normal circumstances, mother and child collaborate in very finely coordinated symbiosis during delivery which should be carefully observed with all our professional skills but which should not be disturbed by hasty intervention. In order to make the pregnancy easier for women, above all, between the sixth and seventh month of pregnancy, when the increasing weight of the baby results in a change in the woman’s musculoskeletal system, the following “basic formula” has proved its worth: • Stabilizing grips before, during, and after treatment, well adapted to the present condition of the woman. • Gentle tonifying in the zones of the lower spine, gluteal, and abdominal muscles, intestine, kidneys and bladder, lymphatic system (alternating stroking movements), and diaphragm. • The zone of the uterus can—but need not—be omitted during the first few treatments until the woman’s general response has been reliably assessed. The spontaneous reaction of the baby, for example, in the form of greatly increased intrauterine movements, and the behavior of the mother-to-be provide a useful indication as to whether the dosage was correctly gauged. In the event of overdose, employ stabilizing grips. • As a result of this treatment the bony and muscular area of the pelvis is gradually and evenly expanded and stretched and the baby obtains the natural space which it needs for development and movement. Fig. 22.1 Female pelvic organs in situ and as zones. • This basic “formula” for the proposed zones can either be incorporated into a normal course of treatment or offered as a short, self-contained treatment. • The subsequent phase of rest, of at least 20 minutes’ duration, is of special importance for pregnant women and should be consistently adhered to or even extended, according to individual requirements. Highly irritated and overanxious women often have tiny drops of water spread over large areas of the inside of both heel bones (the zones of the pelvic organs) before beginning treatment. • This indicates that they are unstable and initially need ample stabilizing grips. Specific treatment of the zones is only gradually built up in the course of a series of treatments according to the increasing stability of the autonomous nervous system. • Every treatment session is interspersed with regularly repeated sedating grips, including in the zone of the solar plexus. Gentle, vibrant tonifying in the sense of regulation in this zone has a similar effect, in our experience. • With these oversensitive women it has proved effective to initially treat them with their feet covered so that they do not feel directly “attacked.” RTF treatment during pregnancy is usually greatly appreciated by most women as they experience its benefits in terms of improvement in their physical complaints and frame of mind. The zones specified below can be supplemented or reduced, depending on the women’s individual histories of complaints. Important note: In most of the indications mentioned below, the lower medial and lateral edge of the calcaneus and lateral malleolus should be treated with the sedating grip as they include the zones of the pelvic tendons and ligaments. The specific treatment of these zones provides great relief and more space (Chapter 28). Gentle, alternating stroking movements, especially in the zones of the thighs, are appreciated by all women as a very effective means of decongestion, not only for the legs, but also for the entire abdomen and pelvis. Stabilizing grips are the first choice. Sedating grips in the zones of the stomach, including the cardia (often the most important) and pylorus, ileocecal valve, solar plexus, central thoracic spine, diaphragm and liver. After improvement of the symptoms these zones may be gently tonified. Tonifying the zones of the small intestine and rectum/anus, including the pelvic floor and spleen, usually brings about spontaneous relief. This short treatment may be performed several times a day, by a partner or another carer if appropriate, in particular in the zones of the stomach and solar plexus. The more advanced the pregnancy, the more frequently many women complain of backache. With acute pain, we apply the rules of treatment in acute situations, as specified for patients with lumbar pain (Chapter 16 and Chapter 21.3.2, section on “Lumbar Syndrome”). Pregnant women with backache can decide for themselves in which position they are able to lie on the treatment table, for example, on one side or even almost seated. If they are starting to suffer from inferior vena cava syndrome (lying flat on their back, the baby causes compression of the inferior vena cava, possibly impairing the mother’s circulation distinctly), we position them on their left side. In this position we can usually apply stabilizing grips quite easily and continue to work. The zones of the lateral abdominal muscles (antagonists of the lumbar spine) are of special importance because as the girth expands increased excess tensions can arise. Sedating grips for the zones of the lower spine and sacroiliac joint are appropriate. Later, they can be gently tonified.
22.1 General Information
22.2 Treatment during Pregnancy
22.2.1 Basic Treatment
Additional Practical Advice
22.2.2 Common Complaints
Vomiting and Nausea during Pregnancy (Hyperemesis gravidarum)
Backache
Musculoskeletal Key
Fastest Musculoskeletal Insight Engine





