Preaxial and Postaxial Polydactyly
Robert Carrigan
DEFINITION
Polydactyly refers to having greater than the normal number of digits.
Preaxial polydactyly is duplication or splitting of the thumb.
Central polydactyly is duplication of the central digits (index, middle, and ring).
Postaxial polydactyly is duplication of the small finger.
ANATOMY
In cases of digit duplication, one may observe duplication in some or all of the elements of the finger (bone, nail, joints, and tendon). The duplicate finger may be well formed and near normal in appearance or underdeveloped and rudimentary in appearance.
Wassel published a classification of thumb duplication based on the work of Adrian Flatt, MD (Table 1).
Postaxial polydactyly classification
Type A: well-formed duplicate small finger with bone or tendon attachments (FIG 1)
Type B: small pediculated nubbin
PATHOGENESIS
Duplication of the digits occurs early in embryogenesis.
Patterning of the limb is demonstrated in three axis: proximodistal axis (modulated by the apical ectodermal ridge [AER]), anteroposterior axis (modulated by the zone of polarizing activity [ZPA]), and the dorsoventral axis regulated by the Engrailed 1 protein (EN1).
Abnormal or ectopic presence of sonic hedgehog protein is implicated in preaxial polydactyly.
Familial cases of postaxial polydactyly demonstrate a defect in the GLI3 gene.
Table 1 Wassel Classification of Thumb Duplication | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
PATIENT HISTORY AND PHYSICAL FINDINGS
The diagnosis of polydactyly is straightforward, clinical examination and radiographs are sufficient to make the diagnosis.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Standard radiographs (three views—anteroposterior, lateral, and oblique) of the hand and affected digit are sufficient to determine the area of involvement (FIG 2).
Advanced imaging such as magnetic resonance imaging (MRI) and computed tomography (CT) is rarely needed.
DIFFERENTIAL DIAGNOSIS
Associated syndromes should be screened for, including trisomy 21 and Rubinstein-Taybi, Apert, and Russell-Silver syndrome.
NONOPERATIVE MANAGEMENT
Observation may be considered for duplicated digits that do not impair function of the hand.
SURGICAL MANAGEMENT
Preoperative Planning
Timing of surgery is variable.
Type B postaxial polydactyly may be removed in the office under local anesthesia, when the child is just a few weeks old.
Preaxial polydactyly reconstruction and type A postaxial reconstructions are elective procedures and are generally performed after 1 year of age and before the start of school.
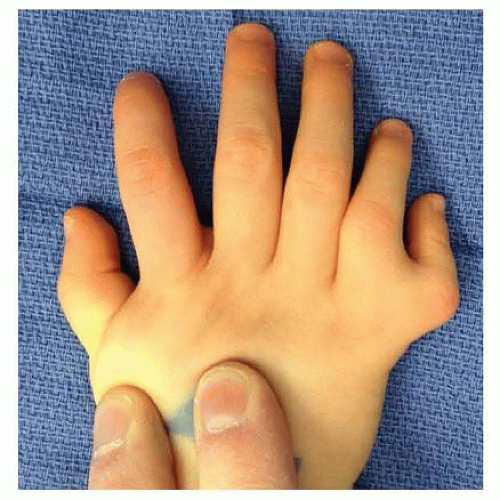 FIG 1 • Type A postaxial polydactyly. |
 FIG 2 • Preoperative radiograph of the patient in FIG 1 with type A postaxial polydactyly, depicting the bifacet metacarpal head. |
Positioning
The patient is positioned supine on the table and the body is pulled over to the affected side.
The arm is placed on a radiolucent hand table and an arm tourniquet is applied.
Approach
Deletion and reconstruction of a polydactyly is not simply an amputation. The surgeon should be aware of protecting and preserving vital structures such as the collateral ligaments and tendon insertions for reattachment to the preserved digit.
Several approaches may be considered for the management of pre- and postaxial polydactyly.Related posts:
 Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
 Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
Arthroscopic Treatment of Chondral Injuries and Osteochondritis Dissecans
 Fragment-Specific Fixation of Distal Radius Fractures
Fragment-Specific Fixation of Distal Radius Fractures
 Arthroscopic and Open Triangular Fibrocartilage Complex Repair
Arthroscopic and Open Triangular Fibrocartilage Complex Repair
 Carpal Tunnel Release: Endoscopic, Open, and Revision
Carpal Tunnel Release: Endoscopic, Open, and Revision
 Surgical Treatment of Acute and Chronic Paronychia and Felons
Surgical Treatment of Acute and Chronic Paronychia and Felons

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


