Section 2 Practical Guidelines for Injection Therapy
Overview
In this section we emphasize the necessity of being able to fully understand the information the patient is imparting in the history, to clearly interpret the signs and symptoms elicited in the examination and finally, to eliminate the various differential diagnoses to arrive at a definitive diagnosis. Only in this way can one successfully achieve the desired result of selecting the patient who might respond to injection therapy (Table 2.1). This, combined with an in depth knowledge of functional anatomy, should enable the clinician to help relieve the many patients with pain from musculoskeletal lesions.
Table 2.1 Indications for corticosteroid injections, with or without local anaesthetic
How to use this book
Equipment
Syringes
All needles and syringes must be of single-use disposable type and must be checked to ensure they are in date. Have available 1 ml, 2 ml, 5 ml, 10 ml and 20 ml sterile syringes; occasionally a 50 ml syringe might be necessary for aspiration (Table 2.2).

The drugs
Local anaesthetic
Lidocaine with epinephrine, which comes in ampoules or vials clearly marked in red, should not be used because of risk of ischaemic necrosis in appendages (page 16). Because of its potential half life of 8 hours or more, we do not recommend the routine use of Marcain but occasionally it can be used when a longer anaesthetic effect is needed. Some practitioners like to mix short- and long-acting anaesthetics to gain both the immediate diagnostic effect and the longer therapeutic effect.
Dosages
It is important to keep within the recommended maximum doses of local anaesthetic in order to avoid toxicity. The safe maximum doses we suggest are given in Table 2.3. These doses are half the maximum published in pharmacological texts, so are well within safety limits (BNF).
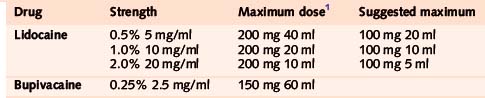
In practice, this translates to the following:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


