Standing posteroanterior and lateral radiographs should be obtained whenever possible.
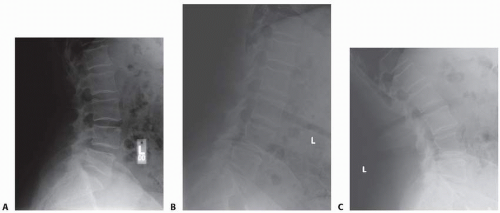
Additional flexion-extension views may provide insight into subtle instabilities (FIG 1).
Full-length posteroanterior and lateral radiographs are obtained in cases of spinal deformity to assess for global balance (coronal or sagittal).
Lateral bending views can help determine the flexibility of the curve and levels for fusion.
Axial computed tomography (CT) images can provide invaluable information about pedicle morphology, particularly in the setting of deformity.
SURGICAL MANAGEMENT
Indications
Degenerative
Spondylolisthesis
Iatrogenic instability
Discogenic back pain
Pseudarthroses
Adult deformity
Curve progression
Neurologic deficit
Back pain refractory to nonoperative care
Pulmonary compromise secondary to deformity
Coronal or sagittal imbalance
Pediatric deformity
Progressive scoliosis more than 50 degrees
Kyphosis more than 75 degrees
Curve progression despite bracing in a skeletally immature individual
Isthmic spondylolisthesis more than 50%
Table 1 Pedicle Morphology
Region
Thoracic
Lumbar
Sacral
General Points
Size
Width increases cephalad and caudal to T5.
T5 is the smallest pedicle (mean 4.5 mm).
Width decreases moving cephalad
S1 pedicle is the widest of all pedicles (mean 18 mm).
Narrowest in mediolateral dimension
Horizontal angulation
Medial angulation increases gradually to 30 degrees at T1.
T12 is angled laterally; T11 is neutral.
Medial angulation increases to 30 degrees at L5.
Angulation is 10 degrees medial at L1.
Angulation is medial at all levels except T12.
Vertical angulation
Angulation increases gradually to T2, then slightly decreases.
There is a large increase in superior angulation between L1 (2 degrees) and T12 (10 degrees).
L5 is angled slightly inferior.
L3 and L4 are neutral.
L1 and L2 are angled slightly superior.
Length
Pedicles become shorter cephalad and caudal to T8.
Longest pedicle is at T8 (45 mm).
Average length is 50 mm throughout the lumbar spine.
There is a high standard deviation in the length of T12 pedicle.
Preoperative Planning
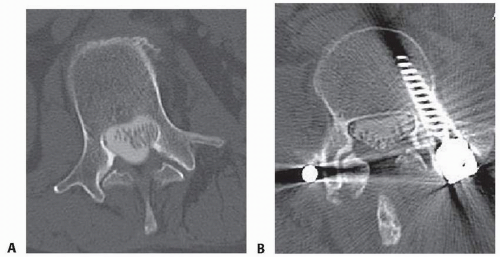
Pedicle anatomy can be best assessed on CT (FIG 2).
A general assessment whether a pedicle is instrumentable can be gained by examining its size on an anteroposterior radiograph of the pedicle.
Pedicle diameter/length and starting points can be determined from the axial image.
Positioning
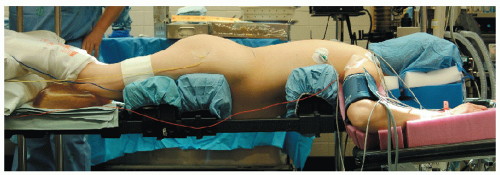
Patients should be placed in the prone position on a radiolucent table (FIG 3).
Care is taken to ensure that the neck is in a neutral position and is not hyperextended.
The arms are positioned at 90 degrees or less of abduction to minimize the likelihood of rotator cuff impingement. The arms are allowed to hang down slightly in a forward-flexed position approximately 10 degrees. The axilla should be clear from any padding to prevent a brachial plexus palsy from occurring.
Elbow pads are placed along the medial epicondyle to protect the ulnar nerve.
The chest pad is placed just proximal to the level of the xiphoid process and distal to the axilla. In women, care is taken to tuck the breasts and ensure that the nipples are pressure-free.
The iliac pads are placed two fingerbreadths distal to the anterior superior iliac spine, allowing the abdomen to hang free and reducing any unnecessary epidural bleeding.
Proper placement of the chest and iliac pads allows for optimal restoration of sagittal alignment via gravity.
FIG 1 • A-C. Flexion and extension lumbar lateral spine radiographs can show evidence of spondylolisthesis as seen here at the L4-L5 level.
FIG 2 • A,B. Pedicle anatomy for screw placement can be assessed with CT scan.
Approach
Two approaches are used: the midline approach and the paraspinal approach.
The midline approach is used for most spinal procedures as it allows direct access to the spinal canal.
The paraspinal approach, also known as the Wiltse approach, was initially described for spondylolisthesis but is also used for far lateral discectomies and minimally invasive musclesparing techniques (eg, minimally invasive pedicle screw instrumentation or transforaminal lumbar interbody fusion).
Specific screw entry points are detailed in Table 2.
FIG 3 • The patient is positioned prone on the Jackson frame.
Table 2 Pedicle Screw Starting Points
Region
Starting Point
Proximal thoracic (T1-T3)
Junction of the midpoint of the transverse process and the lateral pars
Midthoracic (T4-T9)
Junction of the proximal transverse process and the lateral third of the superior articular process
Distal thoracic (T10-T12)
Junction of the midpoint of the transverse process and the lateral pars
Lumbar
Junction of the midpoint of the transverse process and 2 mm lateral to the pars
Sacral
At the inferolateral aspect of the L5-S1 facet joint
TECHNIQUES
▪ Thoracolumbar Pedicle Screw Placement
Pedicle Start Point
Once the bony anatomy of the dorsal elements is meticulously exposed, the proper position of the pedicle entry point is defined. Anatomic landmarks include the lateral edge of the facet joint, the pars interarticularis, and the transverse processes (TECH FIG 1A).
The actual pedicle starting point may vary significantly from the commonly quoted “norms” in many patients. What follows are general guidelines. Preoperative imaging studies (such as CT scan or even the relationship between the pedicle and the lateral aspect of the pars on an anteroposterior radiograph) can provide clues about anatomic variations in a given patient or level.
Only gold members can continue reading. Log In or Register to continue