Posterior Exposure of the Thoracic and Lumbar Spine
Wudbhav N. Sankar
John M. Flynn
DEFINITION
Scoliosis is a three-dimensional deformity of the spine and rib cage.
The hallmark of scoliotic spines is curvature in the coronal plane along with abnormal curvature in the sagittal plane (eg, lordoscoliosis in adolescent idiopathic scoliosis) as well as abnormal vertebral rotation in the transverse plane.
A Cobb angle measurement of greater than 10 degrees distinguishes minor spinal asymmetry from true scoliosis.
The posterior approach to the thoracic and lumbar spine takes advantage of the segmental innervation of the posterior spinal musculature to obtain an internervous and intermuscular plane to provide access to the posterior elements of the spine.
The posterior approach is the most commonly used route for spinal fusion and instrumentation in the scoliotic spine.
ANATOMY
Surface landmarks in the prone position
The vertebra prominens (C7) is typically the most prominent bony structure palpated at the base of the neck.
The superior angle of the scapula is at the level of the T3 spinous process.
The scapular spine is at the level of the T4 spinous process.
The inferior angle of the scapula is at the level of the T7 spinous process.
With the patient in the prone position, the iliac crests are palpated with the fingers and the thumbs brought together at the midline, where they typically overlie the L4-L5 interspace.
The posterior superior iliac spines are at the level of the L5-S1 interspace.
Posterior spinal musculature is divided into superficial and deep layers. The superficial layer, also known as the erector spinae, is composed of the iliocostalis, longissimus, and sacrospinalis muscles. The deep layer consists of the short rotators (multifidus and rotatores) as well as the intertransversarii and interspinous muscles (FIG 1A,B).
Segmental innervation of spinal musculature
Provided by the dorsal rami of the thoracolumbar nerve roots
Segmental blood supply
The posterior intercostal arteries branch from the aorta and subsequently send a dorsal branch posteriorly to the spinal musculature. On its way past the neural foramina, the spinal artery branches off and is sent through the foramina. The spinal artery then divides into anterior and posterior radicular branches within the spinal canal, ultimately supplying the anterior and posterior spinal arteries. Care should be taken to cauterize the branches that lie adjacent to the lateral aspect of the facet (FIG 1C).
In the scoliotic spine, there is rotation of the vertebral bodies in the transverse plane with the spinous processes rotating toward the concavity of the curve.
In the scoliotic spine, the pedicles on the concave side are shorter and have a smaller diameter.5
PATHOGENESIS
Idiopathic
Congenital
Failure of formation or segmentation of vertebral precursors leading to asymmetric vertebral growth with subsequent abnormal curvature
Neuromuscular
Variety of etiologies, such as cerebral palsy, muscular dystrophy, polio, spinal muscular atrophy, and myelomeningocele
Related to an inability to provide muscular support to the spinal column
NATURAL HISTORY
Idiopathic
Infantile (0 to 3 years of age)
Less than 1% of all cases of idiopathic scoliosis
More common in boys
Left thoracic curves predominate
Most resolve spontaneously
Juvenile (3 to 10 years of age)
Eight percent to 16% of all cases of idiopathic scoliosis
More even female-male ratio
Bracing may correct some curves.
Curves of more than 30 degrees usually progress to surgery.
Adolescent (10 to 18 years of age)
Most common form of idiopathic scoliosis
Etiology and pathogenesis are not well understood.
Family history is positive in 30% of cases but does not predict curve magnitude or progression.
More common in girls. The female-male ratio is 1.4:1 for curves 11 to 20 degrees and increases to 5:1 for curves greater than 20 degrees.
Curves have the greatest chance of progression in the period of peak growth velocity leading up to skeletal maturity (prior to menses in females), after which the potential decreases significantly.1
Scoliotic curves measuring less than 20 degrees are at lower risk for progression.
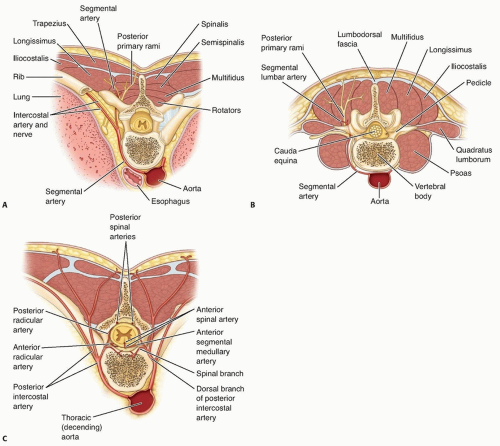
FIG 1 • A,B. Cross-sections of paraspinal musculature. C. Overview at the level of the lumbar spine. The segmental artery courses posteriorly, adjacent to the vertebral body toward the posterior spinal musculature. On passing the neural foramen, the vessel sends a branch through the neural foramen to supply the spinal cord. The vessel continues toward the posterior spinal musculature arising between the transverse processes during the surgical approach where it is prone to bleed.
Scoliotic curves measuring greater than 50 degrees are at higher risk for further progression during adult life (with a percentage of these progressing at a rate of about 1 degree per year).9
There are no significant differences in the prevalence of back pain between adults with scoliotic spines and the general population.7, 10
Scoliotic curves measuring greater than 100 degrees have an increased prevalence of cardiopulmonary compromise (eg, cor pulmonale, restrictive lung disease).6
Congenital
Severity of deformity related to type and location of anomaly
Highest chance of curve progression with unilateral unsegmented bar with contralateral hemivertebrae (nearly 100%), followed by a lone unilateral unsegmented bar, double convex hemivertebrae, single convex hemivertebrae, and finally the block vertebrae3
Neuromuscular
Most curves are progressive and are more difficult to manage nonoperatively.
Curves can cause pelvic obliquity and sitting problems in nonambulatory individuals.
PATIENT HISTORY AND PHYSICAL FINDINGS
Complete history, including age at onset, timing of growth spurts, menses, presence of pain, family history of scoliosis, nerve, or muscle diseases
A complete examination is important to obtain a diagnosis because certain etiologies can predispose the patient to increased operative risk (eg, cardiac abnormalities in patients with Marfan syndrome).
The skin is inspected for café-au-lait spots, the axilla for freckling, and the lumbosacral area for sinus tracts, hairy patches, or dimples. Axillary freckling and multiple café-aulait spots are associated with neurofibromatosis. Sinus tracts,
hairy patches, or dimples in the lumbosacral area are associated with intraspinal anomaly.
The Adams forward bending test detects curvatures by physical examination. Abnormalities in vertebral rotation become apparent as an asymmetric rib hump, prominence, or fullness, leading to possible identification of patients at risk for having scoliosis.
Any shoulder or scapular asymmetry is noted. It is important to point out to parents that this is not always corrected by surgery.
Pelvic obliquity can indicate a possible leg length discrepancy that can mimic a lumbar scoliosis.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



