(1)
Department of Orthopedic Surgery Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Abstract
Most talar osteochondral defects are treated by means of an anterior approach. However, lesions located in the most posterior one third of the talus or osteochondral defects in the posterior tibial plafond can better be treated by means of a two-portal hindfoot approach with the patient in the prone position. The considerations, preoperative planning, and operative approach are described in this chapter.
Most talar osteochondral defects can be treated by means of an anterior arthroscopic approach.
Lesions located in the most posterior one third of the talus or osteochondral defects in the posterior tibial plafond can be treated by means of a two-portal hindfoot approach.
14.1 Introduction
Treatment options for osteochondral defects are diverse. Treatment is most of all guided by the size of the lesion. The primary surgical treatment of defects up to 15 mm in diameter consists of arthroscopic debridement and bone marrow stimulation.
Preoperatively it has to be decided how to approach the defect. Depending on the preference of the surgeon and the location of the lesion, the approach can be from the front, from the back, or by means of a malleolar osteotomy. In case of arthroscopic treatment, it has to be decided to treat the osteochondral defect by full plantar flexion in the anterior working area, with the ankle in the neutral position and using soft tissue distraction, or to approach the lesion from posterior. Most lesions can be treated by means of an anterior approach. Lesions located in the most posterior one third of the talus can best be treated by means of a two-portal hindfoot approach.
14.2 Preoperative Planning
Routine radiographs of the ankle can disclose the lesion, but usually it needs an MRI or better a CT scan. For preoperative planning, a CT scan provides important information (Reilingh et al. 2009). The multislice helical CT protocol involves actual 0.5-mm acquisition with 0.3-mm reconstruction. Multiplanar coronal and sagittal reconstruction should be 2 mm.
If the osteochondral defect on the sagittal reconstruction is located extremely posterior, it can be decided to approach the lesion from posterior. In general 95 % of all osteochondral lesions in the ankle can be approached from anterior. Only the very posterior talar lesion can be approached from posterior.
Osteochondral defects in the tibial plafond are often located in the posterior part of the joint. They can be approached from posterior.
14.3 Operative Technique
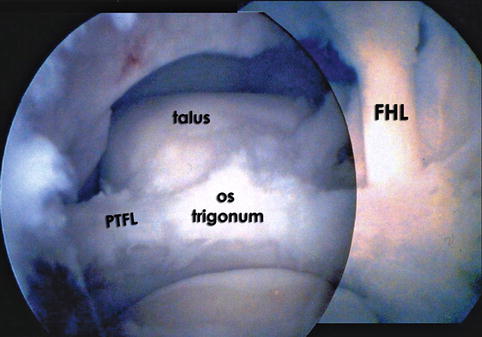
The patient is placed in the prone position. The routine two-portal hindfoot approach is used (see Chap. 12). After opening the joint capsule of the ankle joint, the talar dome can be inspected. Applying a soft tissue distractor is useful at this point (Figs. 14.1, 14.2 and 14.3). The defect is probed and unstable cartilage is removed by means of the probe, curette, or shaver (Fig. 14.4). After debridement multiple connections with the subchondral bone are created. This can be accomplished by the microfracture probe. The objective is to partially destroy the calcified zone and to create multiple openings in the subchondral bone. Intraosseous blood vessels are disrupted and the release of growth factors will lead to formation of a fibrin clot. The formation of local new blood vessels is stimulated, marrow cells are introduced in the defect, and fibrocartilaginous tissue is formed (Fig. 14.5). All unstable cartilage should be removed (Figs. 14.5 and 14.6).