Placement of Thoracic Pedicle Screws
Patient Selection
Indications
Advantages of thoracic pedicle screw fixation—Achieves stable three-column fixation, improves control of three-dimensional deformities
Degenerative disorders
Traumatic injury
Deformity
Stabilization of spinal segments
After neural decompression for fracture, tumor, infection
Facilitate correction of kyphotic or scoliotic deformities
Contraindications
Signs or symptoms of infection
Metal allergies
Severely deformed, hypoplastic, or absent pedicles
In trauma setting, medically unstable or underresuscitated patients
Severe osteoporosis (relative); address inadequate screw purchase with screw augmentation techniques such as polymethyl methacrylate screw augmentation
Preoperative Imaging
AP and lateral radiographs
CT optional to evaluate pedicle size and anatomy of deformity; assessment of pedicles at rotated levels may be impossible on plain radiographs; if pedicle size appears too small to accept 5-mm screw or plain radiography examination is insufficient, use CT for accurate evaluation
Pedicles in midthoracic spine have smallest width in patients of all ages; pedicles at apices of concavity of scoliotic curve typically smaller than those on convex side
Can safely insert screws 80% to 115% of size of outer pedicle diameter through gradual plastic deformation, in a technique known as pediculoplasty, with probe and tap; this deformation is more pronounced in pediatric pedicles
Procedure
Room Setup/Patient Positioning
Prone position on radiolucent four-poster frame or OSI table (Orthopaedic Systems) with spine top
Move patient down toward foot of operating table as much as possible so arm boards can be close to head of table; improves surgeon access while placing screws in proximal thoracic spine
Place legs in sling to promote systemic venous return
Consider halo skull traction to facilitate flexing patient’s neck and reduce kyphotic angle for easier screw placement
Use somatosensory-evoked potentials and motor-evoked potentials to monitor spinal cord during screw insertion and correction maneuvers
Real-time spontaneous electromyography (EMG) monitoring of nerve roots T6 through T12 through the rectus abdominis musculature adds layer of safety; can use triggered EMG to confirm screw placement
Special Instruments/Equipment/Implants
Fluoroscopic and computer-generated image–guided techniques developed to improve pedicle screw placement accuracy require additional resources; may increase surgery time, blood loss, and infection
Thoracic gearshift probe
Flexible ball-tipped pedicle-sounding device
Variety of screw sizes—4 to 7 mm in diameter; 25 to 55 mm in length
Monoaxial screw heads allow better manipulation of spine during derotation
Polyaxial screws aid rod placement after curve correction
Uniaxial screws combine benefits of monoaxial and multiaxial screw heads
Surgical Technique
Incision and Exposure

(Reproduced with permission from Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew KD : Free hand pedicle screw placement in the thoracic spine: Is it safe? Spine [Phila Pa 1976]2004;29[3]:333-342.)
Mark incision from highest planned instrumented vertebra to lowest; make straight vertical line connecting the two points to ensure straight incision after scoliosis correction and confirm with fluoroscopy
For exposure, incise from spinous process above most cranial vertebra to spinous process of most caudal vertebra to be instrumented
Anesthesia team paralyzes patient pharmacologically to facilitate exposure of soft tissues; reverse paralysis before instrumentation to avoid interfering with monitoring
Carry dissection along midline; dissect subperiosteally laterally to tips of transverse processes (Figure 1)
Perform wide facetectomy; use osteotome to remove inferior 3 to 5 mm of inferior facet; scrape exposed cartilage from superior facet
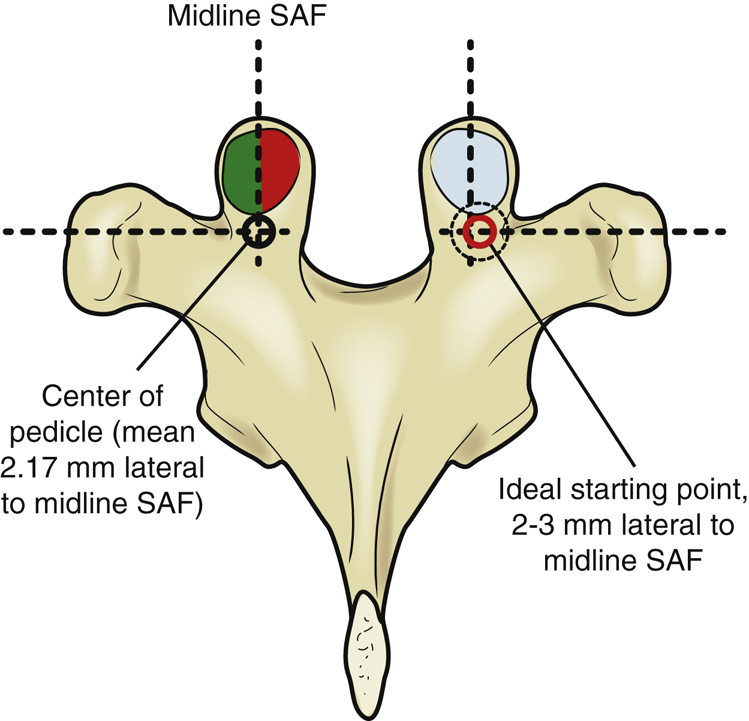
Starting Point and Trajectory
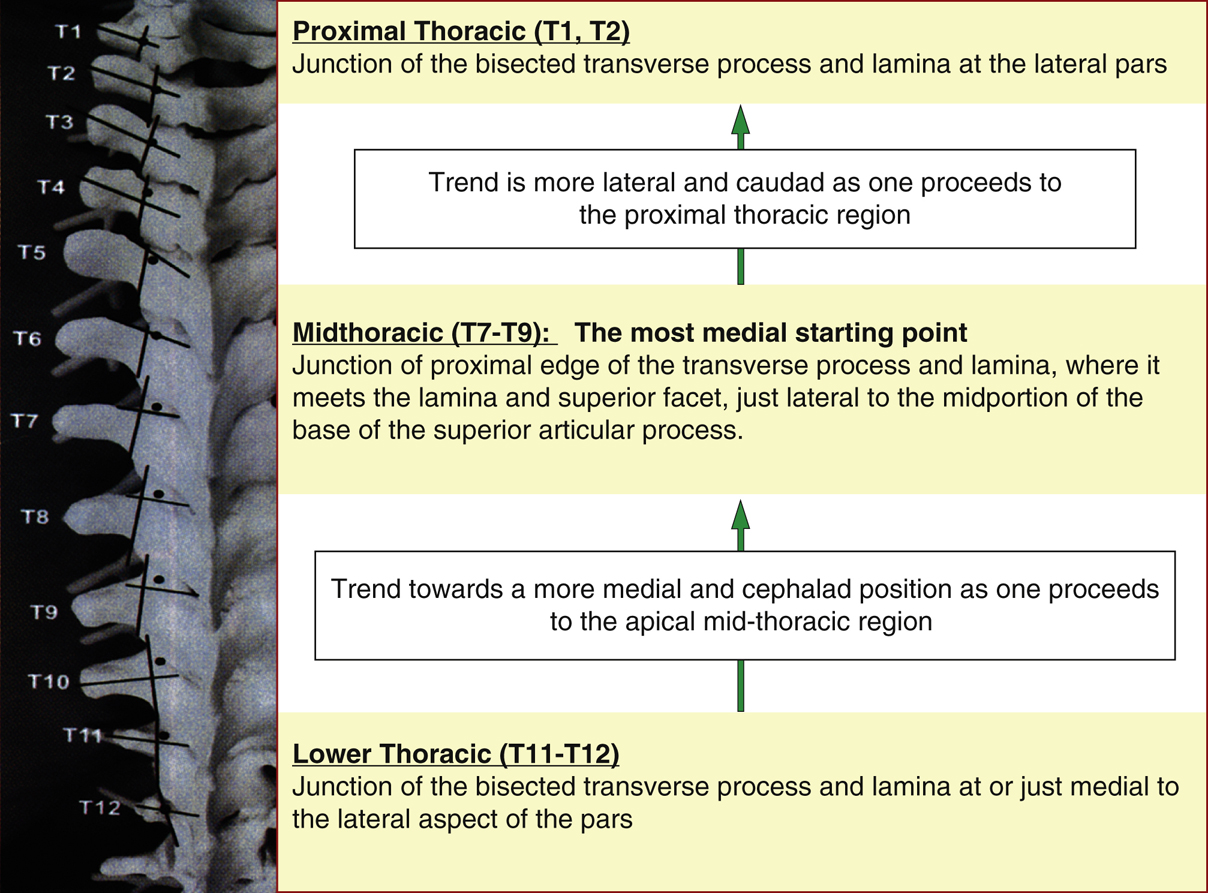
Figure 2Image shows pedicle screw starting points using a 3.5-mm acorn-tipped burr. The posterior elements are burred to create a posterior cortical breach approximately 5 mm in depth.
(Adapted with permission from Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew KD : Free hand pedicle screw placement in the thoracic spine: Is it safe? Spine [Phila Pa 1976]2004;29[3]:333-342.)