Pediatric fractures—introduction
Introduction
Special features of pediatric fractures
Children are not small adults. Their behavior in response to trauma is different from that of an adult as a result of their size and physiology, the physical properties of the skeleton as well as its capacity to heal with remodeling and growth. The major difference in the pediatric skeleton is the presence of growth plates, and a thicker periosteum than in adults, which has a more active healing capacity, is less readily torn, and is capable of being more easily stripped from the bone. The thicker periosteum usually helps to hold fractures and maintain alignment, contributing to faster fracture healing than in adults. However, growth plate injuries and epiphyseal injuries can lead to growth disturbance that may result in limb-length discrepancy and deformity.
In addition, children‘s bones are less dense than adult bones. They are also more porous as a result of increased penetration of vascular channels. Pediatric bone has a comparatively lower modulus of elasticity, with lower bending strength and lower mineral content. For these reasons, bone in children can easily fail either in tension or compression.
General principles in treating pediatric fractures
The general principles of pediatric fracture care are to:
Relieve pain
Restore anatomy and function with early return to activity (mobilization)
The type of treatment should be appropriate to the child‘s age and type of injury. Similarly, the same AO principles of operative fracture care that apply to adults, apply to fractures in children:
Anatomical reduction of displaced articular injuries as well as growth plate injuries, and anatomical alignment to restore axis, length, and rotation in diaphyseal/metaphyseal fractures
Stable fracture fixation: absolute stability for articular injuries and relative stability in most diaphyseal injuries
Preservation of blood supply: use of minimally invasive techniques
Early mobilization of the limb and patient: early return to function
Indications for operative treatment
When a fracture cannot be reduced and maintained in a satisfactory position by closed means (nonoperative treatment) it should be treated operatively. Spiegel and Mast [ 1] list five principles applicable to the operative management of pediatric fractures:
Multiple closed reductions of an epiphyseal fracture are contraindicated because they may cause repetitive damage to the germinal cells of the physis, thereby predisposing to premature closure and late deformity.
During surgery anatomical reduction is mandatory, especially for displaced intraarticular and epiphyseal fractures.
Internal fixation devices, if used, should be as simple as possible (ie, K-wires) and should be removed as soon as the fracture has healed.
Rigid fixation to allow immediate mobilization of the extremity is not usually the goal; rather the goal is sufficient stability to hold the fragments in anatomical alignment with a supplemental cast if required.
External fixators when used have to be removed as soon as possible, and cast immobilization is substituted when the soft-tissue problems have been treated or when the fracture is stable. However, in a multiply injured patient, the internal or external fixation must be of sufficient strength to allow for mobilization of the child.
Thus, planning for appropriate surgical procedures is based on the age and size of the child, the bone(s) fractured, and the extent and severity of associated injuries.
Indications and contraindications for minimally invasive plate osteosynthesis (MIPO) in pediatric fractures
Indications for MIPO:
Complex long-bone fractures of the lower extremity that are not suited to treatment with elastic nails in children older than 10 years, or overweight
Some corrective osteotomies of the lower extremity
Contraindications for MIPO:
Fractures of the upper extremity
Severe soft-tissue injuries associated with lower extremity fractures (MIPO can be performed after the soft-tissue injury has improved)
Epiphyseal injuries
Intraarticular injuries
Surgical anatomy
Femoral shaft
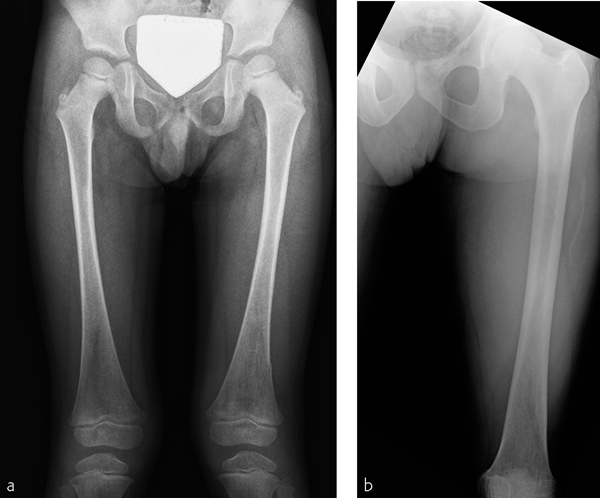
The difference in children when compared to adults concerning the femoral shaft is the proportion in length and size of the bone compared with the adult. The other concern is injury to the epiphyseal plate at both ends when using a long plate or insertion of the pin for indirect reduction ( Fig 23.1-1 ).
The most important aspect of treating children with a fracture is respecting the physis. Therefore, the use of intraoperative imaging (C-arm) is mandatory to avoid injury to growth plates when using screws at the end of the plates, or when using the different reduction techniques with distractors, external fixators, or elastic nails.
For general information on the surgical anatomy of the femur, shaft, see chapter 17.1, Femur, shaft—introduction; and for tibia and the fibula, shaft, see chapter 20.1, Tibia and fibula, shaft—introduction.
Preoperative assessment
General information about the patient
In children, preoperative assessment of the patient includes consideration of age, size, weight, isolated or multiple fractures, monotrauma or polytrauma, and differential diagnosis of physical child abuse.
In polytrauma pediatric patients, advanced trauma life support (ATLS) protocols should be followed. Fracture assessment should include soft-tissue condition (open, closed, compartment syndrome), fracture location, and configuration. Possible injuries to the growth plates, metaphysis, or epiphysis should be excluded. The neurological and vascular status should be examined in all fractures.
Type of x-rays and CT scans
Conventional x-rays with two orthogonal views are sufficient for shaft fractures. In cases where the fracture involves the growth plate, comparative x-rays from the uninjured side are useful. In cases of articular injury, the use of CT scans will help in the decision-making process.
Choice of implants
For MIPO the choice of implants depends on the patient‘s bone size. Conventional plates and screws can usually be used. However, if particular conditions exist, such as osteopenia, severe comminution, short proximal or distal fragments, the use of locking plates should be considered.
Related posts:
 Clavicle—introduction
Partially unstable pelvic ring injury: bilateral anterior pubic root fractures and a disruption of the left sacroiliac joint—61-B2.2
Pelvis, acetabulum: both-column acetabular fracture—62-C2 and 62-C7 body fracture
Femur, proximal: extraarticular fracture, intertrochanteric—31-A3 and wedge diaphyseal fracture—32-B1
Tibia and fibula, proximal: intraarticular bicondylar fracture, no metadiaphyseal involvement—41-C3
Tibia and fibula, shaft—introduction
Clavicle—introduction
Partially unstable pelvic ring injury: bilateral anterior pubic root fractures and a disruption of the left sacroiliac joint—61-B2.2
Pelvis, acetabulum: both-column acetabular fracture—62-C2 and 62-C7 body fracture
Femur, proximal: extraarticular fracture, intertrochanteric—31-A3 and wedge diaphyseal fracture—32-B1
Tibia and fibula, proximal: intraarticular bicondylar fracture, no metadiaphyseal involvement—41-C3
Tibia and fibula, shaft—introduction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


