Figure 6.1
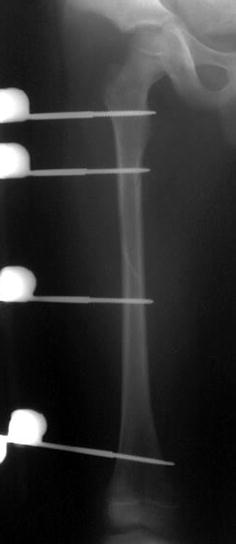
Skeletal traction with distal femoral traction pin
Immediate hip spica casting.
Delayed hip spica casting after 10–14 days.
Deciding on the type of fixation also varies with age. An algorithm to help decide accordingly is summarised in Table 6.2. Options include:


Each technique has advantages and disadvantages and a number of factors need to be considered to determine the most appropriate option for managing paediatric femoral fractures (See Table 6.1).
Table 6.1
Management options, tips, advantages and disadvantages
Method | Age | Technical tips | Recommended | Contraindicated | Advantages | Disadvantages | |
|---|---|---|---|---|---|---|---|
Pavlik harness | <6 months | Ensure parents understand residual displacement will remodel | Proximal and middle third | Distal fractures, >6 months | Avoids skin irritation from spica cast | If > 20° angulation deformities reliant on remodeling | |
Immediate spica casting | 6 months–5 years | Close follow-up first 3 weeks, cast wedging to correct angulation deformity | Low energy, isolated fractures. Where telescope test results in less than 30 mm shortening | Multiple trauma, Obesity | Simple, proven history | Prolonged immobilization. Assessment of soft tissues and Skin loss Loss reduction | |
Traction and casting | 6 months–5 years 5–10 years low energy | Traction pin inserted medial to lateral 90°–90° traction. Hip spica when no fracture site tenderness and radiographic evidence of callus (2-weeks) Traction weight 0.5 kg per year of life | Where shortening unacceptable for immediate casting. In increasing age or higher energy | Obesity Floating knee Head injury Polytrauma Distal fractures | Non-invasive. | Prolonged hospital stay. Outdated with internal fixation techniques | |
Flexible nailing | 5–12 | Nail diameter 40% isthmus femur. Use nails of the same diameter | Transverse, short oblique fractures | Very proximal or very distal spiral fracture. Length unstable >49 kg | Early mobilization, avoids physis, reduced re-fracture. | Skin tip irritation, malunion/shortening in unstable fractures, proximal or distal fracture may require limited weight bearing or bracing | |
External fixation | 5–16 | Release TFL to allow knee movement | Severely injured, large soft tissue defect, wide area fracture comminution. If nailing or plating contraindicated | If amenable to nailing | Minimally invasive, quick, early weight bearing | Refracture following removal, pin site infection, knee stiffness, family and schooling stigma with frame. Delayed union. Construct too rigid for callus formation but reduction not stable enough for primary bone healing | |
Compression plating | 5–16
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





