Fig. 4.1
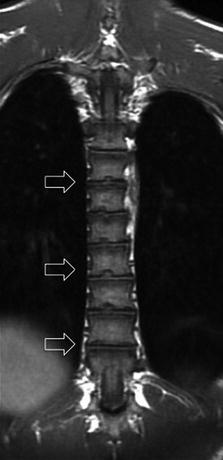
Fig. 4.2

Fig. 4.3
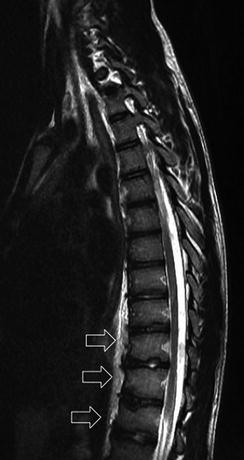
Fig. 4.4
A 14-year-old male soccer player complained of pain along the thoracolumbar spine which had increased with hyperextension maneuvers. Spondylolysis was initially suspected so an MRI of the lumbar area was performed. Image findings indicated a new study of the thoracic spine.
Comments
Osteochondrosis is a family of joint orthopedic diseases occurring in children and adolescents. Scheuermann’s disease is considered a form of spinal juvenile osteochondrosis. It consists of a thoracic/thoracolumbar hyperkyphosis due to wedged vertebrae.
The true incidence of juvenile kyphosis is not known and ranges between 1 and 8 %. The exact etiology is unknown. It has a genetic background and develops due to an ossification disturbance of the vertebral bodies. The front of the upper spine does not grow as fast as the back, so that vertebrae become wedge shaped, with the narrow part of the wedge towards the front.
Pain can arise from postural changes. Cervical and lumbar pain is caused by compensatory hyperlordosis above or below the primary deformity.
There are two types with different diagnostic criteria:
1.
Juvenile kyphosis (type I) or “classic” Scheuermann’s disease
(a)
Wedging of more than 5° in one or more vertebrae in the thoracic or thoracolumbar region
(b)
Disk space narrowing
(c)
End plate irregularities
(d)
Increased thoracic or thoracolumbar kyphosis
Schmorl’s nodes are often associated with juvenile kyphosis but are not a pathognomonic sign.
2.
Juvenile kyphosis (type II, “lumbar”) or atypical Scheuermann’s disease
Obligatory criteria:
(a)
End plate irregularities in one or several vertebral bodies of the lumbar or thoracolumbar area
(b)
Increased sagittal diameter of vertebral bodies (without significant wedging), loss of lumbar lordosis
(c)
Disk space narrowing
Possible criteria:
(d)
Apophyseal separation
(e)
Schmorl’s nodes
Back pain occurs mainly during the day and under loading and is more common in Type II. This atypical Scheuermann’s disease is commonly seen in athletes as a consequence of mechanical overloading.
Idiopathic thoracic hyperkyphosis (“roundback,” “poor posture”) must be differentiated from juvenile kyphosis: clinically, postural thoracic hyperkyphosis is mobile, more harmonic, and not as localized as Scheuermann’s kyphosis. On radiographs, there is no wedge deformation, and disk space height is not decreased. Usually, the deformity corrects on extension.
The definitive diagnosis of juvenile kyphosis can often be made by conventional radiographs alone. However, MRI highlights end plate abnormalities, premature disk degeneration, and vertebral wedging significantly better.
Treatment largely depends on the degree of kyphosis. This soccer player was treated without a brace with physical therapy, mobilization, and strengthening exercises.
Radiological Findings
Sagittal MR FSE T2-weighted image of the lumbar spine (Fig. 4.1) does not reveal pathological findings for spondylolysis. Some irregularities are seen in several vertebral end plates of lower thoracic vertebrae (open arrows). Coronal FSE T1-weighted image (Fig. 4.2) and sagittal FSE T2-weighted images (Figs. 4.3 and 4.4) of the thoracic spine show vertebral end plate irregularities in the T6–T12 segment, slight increase in sagittal diameter of vertebral bodies, disk space narrowing, and normal lumbar lordosis, which are typical of juvenile kyphosis (type II).
Case 4.2: Osteochondrosis of the Apophysis of the Base of the Fifth Metatarsal or Iselin Disease
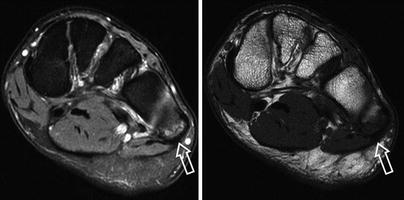
Fig. 4.5

Fig. 4.6

Fig. 4.7

Fig. 4.8
A 16-year-old soccer player presented with localized pain on the lateral aspect of the left foot while training.
Comments
The proximal fifth metatarsal is the insertion site of three ligaments (lateral band of the plantar fascia and plantar and dorsal fourth to fifth metatarsal ligaments) and two tendons (peroneus brevis and peroneus tertius).
Iselin disease is defined as an overuse injury caused by repetitive pressure and/or traction on the growth center at the base of the fifth metatarsal. It is subsequent to the tension produced by the peroneus brevis muscle tendon and is especially found in young athletic males with tight calf muscles. It is often misdiagnosed as a fracture.
The normal apophysis is usually seen between ages 10 and 14. The apophyseal line runs parallel to the shaft of metatarsal along the tubercle’s inferolateral margin. It does not extend proximally into the joint.
Pain is most commonly found along the foot’s outer edge. It worsens with activity and improves with rest. It is usually self-limiting, but if bone maturity is reached and symptoms continue, the injury can develop into a nonunion.
The diagnosis of Iselin disease is made primarily based on the clinical presentation and physical exam. Radiographs are useful to exclude other causes of foot pain. It usually is not visible on anteroposterior or lateral radiographs, but can be seen on the oblique view. They can help in assessing for displacement of the growth center.
Differential diagnosis for fifth metatarsal diseases includes:
Jone’s fracture: transverse fracture at the diaphysis/metaphysis junction. It extends from the lateral aspect of the fifth metatarsal towards the articular surface between metatarsals four and five. It is generally caused by tensile stress along the metatarsal’s lateral border.
Stress fracture of the proximal fifth metatarsal: transverse diaphyseal pathological fracture at the proximal 1.5 cm of the shaft. It is described in Case 4.8.
Avulsion fracture: when the proximal portion of the fifth metatarsal is fractured off secondary to a violent contraction of the peroneus brevis during sudden foot inversion. The fracture line appears in the transverse plane; sometimes it can be slightly oblique.
Os vesalium: accessory bone found proximal to the base of the fifth metatarsal within the peroneus brevis tendon.
Treatment is aimed to reduce pain and inflammation. Depending on symptom severity, treatment may include rest from any aggravating activities; ice massage to the inflamed area; stretching of calf and peroneal muscles; custom foot orthotics to address postural abnormalities and relieve the pressure on the growth plate; and protective, stable footwear to support the foot while the area heals. In our case, this patient (who also had a subchondral cuboid fracture) remained at rest for 38 days.
Radiological Findings
Coronal fat-suppressed MR FSE T2- and PD-weighted images of the foot (Fig. 4.5) reveals edema of the apophysis of the base of the fifth metatarsal (open arrow).
The axial T1 spin eco-weighted image (Fig. 4.6) shows the apophysis (open arrow) and, incidentally, a small subchondral cuboid fracture (arrowhead). The acute cuboid edema and the traction injury at the fifth metatarsal’s apophysis are clearly appreciated in the axial FSE T2 fat-saturated weighted images (Fig. 4.7).
A normal apophysis of another 12-year-old soccer player with fifth metatarsal pain is seen in an oblique plain radiograph (Fig. 4.8).
Case 4.3: Freiberg’s Infraction

Fig. 4.9
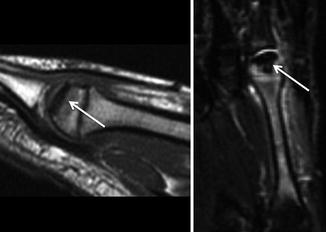
Fig. 4.10
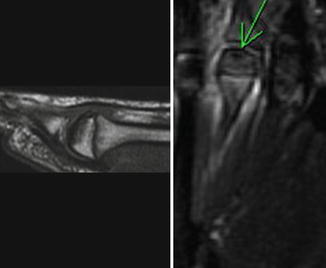
Fig. 4.11
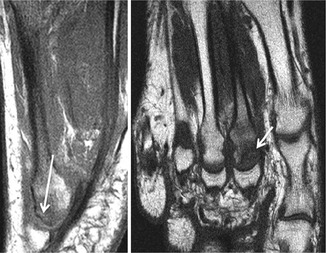
Fig. 4.12
A 16-year-old female rhythmic gymnast suffered from anterior right foot pain during training.
Comments
Freiberg’s infraction is an osteochondrosis (intraarticular) that is preferentially located at the epiphyseal nucleus of the head of the second metatarsal, but can be found, less frequently, at the third metatarsal. The disease progression and imaging are the same as usual for osteochondrosis.
Several synonyms have been used to described Freiberg’s infraction including: Freiberg’s infarction, osteochondrosis of the second metatarsal head, eggshell fracture, Koehler second disease, Panner disease of the metatarsal, osteochondritis deformans metatarso-juvenilis, malacopathia, subchondral bone fatigue fracture of the second metatarsal head, and dorsal fatigue stress injury of the second metatarsal head.
Freiberg’s infraction is a relatively common osteochondrosis of the second metatarsal head. It appears to affect young women who are active in sports. Its etiology is thought to be traumatic in nature causing a painful alteration, subchondral disruption, and collapse of the articular cartilage. “Infraction” is sometimes called Freiberg’s “infarction.” Infarction would suggest a vascular event leading to osteonecrosis. It has been suggested that avascular necrosis from injury will lead to the growth plate or epiphyseal injury in young, growing bone. This may also explain why the incidence is higher in young women and girls. The location and radiographic appearance of metatarsal head subchondral fractures are similar to those seen in Freiberg’s infraction. The term infraction refers to an incomplete fracture of bone without displacement of fragments.
Although Freiberg’s infraction affects adolescents (12–18 years) and metatarsal head subchondral fractures are seen in adults, both entities likely share a cause that combines mechanical stress, subchondral fracture, vascular injury, and subsequent osteonecrosis. Therefore, it is possible that Freiberg’s infraction and metatarsal head subchondral fractures occurring in adults have the same pathogenesis.
Diagnosis is often confirmed by simple radiographs which show varying stages of metatarsal head injury and articular depression. MRI aids in the diagnosis of Freiberg’s infraction before joint changes occur on radiograph. This may be particularly useful in the early stage of the disorder when joint pain is present without observed changes to the joint surface, and MRI can detect edema. There might be incidental detection of asymptomatic osteochondrosis such as the present case on the contralateral foot.
Radiological Findings
Plain radiograph (Fig. 4.9) shows slight sclerosis within the third metatarsal head (arrow) of the right foot. MRI shows significant edema through the third metatarsal with low signal on sagittal T1 and STIR coronal view (Fig. 4.10) within the head of the metatarsal due to necrosis (arrows). Figure 4.11 shows an asymptomatic osteochondrosis on the second metatarsal of the left foot (arrow).
Figure 4.12 depicts a metatarsal head subchondral fracture of a 63-year-old female. Sagittal and coronal T1-weighted images show metatarsal head flattening (long arrow) involving dorsal surface with subchondral sclerosis (short arrow).
Case 4.4: Physeal Widening of the Distal Femur and Proximal Tibia

Fig. 4.13

Fig. 4.14

Fig. 4.15

Fig. 4.16
A 13-year-old male tennis player complains of knee pain during the last 3 weeks without any related traumatic event.
Comments
Physeal widening can be observed on MRI of children as the result of a variety of metaphyseal insults. The widening may be broad or more focal. These areas of physeal widening differ from Salter-Harris type 1 injuries in that no discrete fracture is identified through the cartilage, the widening can be quite focal, and neither epiphyseal nor apophyseal displacement is seen.
Salter-Harris fractures are often the result of an acute insult or injury in children, whereas broad physeal widening is suggestive of chronic stress. This form of repetitive microtrauma results in the equivalent of a stress injury disrupting the microvascular blood supply to the physis, thereby interrupting normal endochondral bone formation. The term “epiphysiolysis” has been used in this respect, especially in the humerus, but it is potentially misleading since it could imply separation of the epiphysis from the proximal shaft or a fracture through the epiphysis itself, neither of which is expected here.
This condition is associated with knee pain but not related to an acute traumatic event, although it is referred with an intense sport activity. Usually these children are high-intensity, competitive elite, or subelite athletes who participate in sports, beyond the recreational level. Extension of physeal signal intensity into the adjacent metaphysis of bones has been described on MRI in both symptomatic and asymptomatic children. The newly formed metaphyseal bone immediately adjacent to the physis is relatively fragile and has poor resistance to compressive forces, such as those from the chronic stress of competitive sports activity. The radiologist may be the first to recognize the physeal widening seen on imaging and to suggest that this finding is a possible form of stress injury in competitive, skeletally immature athletes. MRI in children with overuse pain may be performed to confirm physeal widening detected on radiography and to exclude other injuries that may cause prolonged joint pain.
Treatment is conservative which consists of relative rest with an average period of 3 months.
Case 4.5: Premature Physeal Arrest of the Distal Tibia

Fig. 4.17
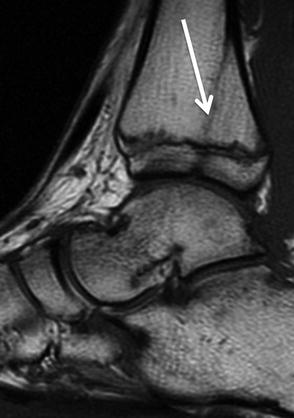
Fig. 4.18

Fig. 4.19
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


