As with most fractures associated with osteoporosis, the incidence of pelvic ring injuries in this population of patients is rising rapidly. Osteoporotic pelvic ring injuries are exceedingly different in their etiology, natural history, and treatment from the more recognizable patterns in young patients with high-energy pelvic ring injuries. Recognition of a potentially unstable fracture pattern, careful evaluation of the ambulatory and functional status of each patient before injury, and the potential pitfalls and benefits of operative versus nonoperative care are critical to the effective treatment.
Key points
- •
Osteoporotic pelvic ring injuries have historically been treated nonoperatively.
- •
Osteoporotic patients are not only elderly, and continue to be active and demanding of a return to ambulatory lifestyles.
- •
Injuries need to be delineated as high-energy versus low-energy.
- •
The implications of injury patterns may be quite different for osteoporotic patients, as ligamentous structures rarely are included as part of their injury spectrum.
- •
Treatment options vary greatly from those typically chosen for young patients.
Incidence
The osteoporotic pelvic ring injury is grossly underrepresented in the reporting of all pelvic ring injuries. Historically most of these injuries were treated nonoperatively, with little attention paid to the individual fracture pattern. The combination of an increasing geriatric population with greater demands for function, and their complex medical comorbidities, makes pelvic ring injuries a life-changing event for each patient. In North America there are no published estimates of the incidence of osteoporotic pelvic ring injuries. Overall the incidence of pelvic ring fractures varies from 0.3% to 8% of all fractures. The force needed to impart a pelvic ring fracture has been estimated at 2000 to 10,000 N on nonosteoporotic bone. This premise alludes to 2 important points: (1) if a high-energy force is delivered to osteoporotic bone, the patient is likely to sustain a significantly worse injury to the soft tissues; and (2) the increasing incidence of pelvic trauma in osteoporotic patients is not secondary to high-energy trauma.
In Finland, from 1970 to 1997 there was a 23% increase in the age-adjusted incidence of pelvic ring in combination with a 6-year increase in the median age of the patients suffering these fractures. This long-term population study suggested that the number of osteoporotic pelvic ring fractures could triple by the year 2030. If this trend is extrapolated to a worldwide estimation, in those countries where osteoporosis is highly prevalent the number of pelvic ring injuries will be staggering. This study also elucidates that the large preponderance of these fractures (83%) was due to a ground-level fall secondary to a multifactorial gait disturbance. This fact needs to be considered in the context of the acute increase, since that time, in numbers of geriatric patients who continue to live active lives (including driving), which will clearly lead to an increase in the incidence of high-energy pelvic ring injuries in parallel with low-energy fractures of the pelvis. Overall this incidence should be reflected in a much more commonly studied fracture, that of proximal femoral fractures (hip fractures). There has in fact been a significant decrease in the overall incidence of hip fractures in the period from 1995 to 2005 according to Medicare databases, with a decline of 24.5% in women 19.2% in men. The suspected cause of the decline is the use of bisphosphonate therapy, and this is a critical finding in these patients, as the number of their comorbid medical conditions continues to increase. It is unknown whether the incidence of pelvic ring fractures is following that of hip fractures; however, it is clear that, similar to the history of hip fracture treatment, the techniques of fixation and rehabilitation needed for osteoporotic pelvic ring injuries must evolve to meet patients’ expectations for an active lifestyle, much as they have for patients with osteoporotic proximal femur fracture.
Incidence
The osteoporotic pelvic ring injury is grossly underrepresented in the reporting of all pelvic ring injuries. Historically most of these injuries were treated nonoperatively, with little attention paid to the individual fracture pattern. The combination of an increasing geriatric population with greater demands for function, and their complex medical comorbidities, makes pelvic ring injuries a life-changing event for each patient. In North America there are no published estimates of the incidence of osteoporotic pelvic ring injuries. Overall the incidence of pelvic ring fractures varies from 0.3% to 8% of all fractures. The force needed to impart a pelvic ring fracture has been estimated at 2000 to 10,000 N on nonosteoporotic bone. This premise alludes to 2 important points: (1) if a high-energy force is delivered to osteoporotic bone, the patient is likely to sustain a significantly worse injury to the soft tissues; and (2) the increasing incidence of pelvic trauma in osteoporotic patients is not secondary to high-energy trauma.
In Finland, from 1970 to 1997 there was a 23% increase in the age-adjusted incidence of pelvic ring in combination with a 6-year increase in the median age of the patients suffering these fractures. This long-term population study suggested that the number of osteoporotic pelvic ring fractures could triple by the year 2030. If this trend is extrapolated to a worldwide estimation, in those countries where osteoporosis is highly prevalent the number of pelvic ring injuries will be staggering. This study also elucidates that the large preponderance of these fractures (83%) was due to a ground-level fall secondary to a multifactorial gait disturbance. This fact needs to be considered in the context of the acute increase, since that time, in numbers of geriatric patients who continue to live active lives (including driving), which will clearly lead to an increase in the incidence of high-energy pelvic ring injuries in parallel with low-energy fractures of the pelvis. Overall this incidence should be reflected in a much more commonly studied fracture, that of proximal femoral fractures (hip fractures). There has in fact been a significant decrease in the overall incidence of hip fractures in the period from 1995 to 2005 according to Medicare databases, with a decline of 24.5% in women 19.2% in men. The suspected cause of the decline is the use of bisphosphonate therapy, and this is a critical finding in these patients, as the number of their comorbid medical conditions continues to increase. It is unknown whether the incidence of pelvic ring fractures is following that of hip fractures; however, it is clear that, similar to the history of hip fracture treatment, the techniques of fixation and rehabilitation needed for osteoporotic pelvic ring injuries must evolve to meet patients’ expectations for an active lifestyle, much as they have for patients with osteoporotic proximal femur fracture.
Anatomy
Pelvic anatomy is composed of innominate and sacral bones along with soft-tissue attachments that, on fracture, act to both stabilize and potentially displace the skeleton. In young patients, low-energy injuries typically result in purely soft-tissue injuries, and osseous injuries are often bony avulsions. In the elderly patient, the bony anatomy typically fails with minimal trauma and the soft tissues (ligaments) rarely fail in significant fashion. Therefore, remarkable fractures of the osteoporotic pelvis may not be markedly unstable. The primary ligaments in the pelvis include the sacrotuberous, sacrospinous, anterior sacroiliac, and posterior sacroiliac. Additional constraints include the pubic symphysis and the iliolumbar ligaments. The vascular anatomy is often calcified as well as compromised in the geriatric osteoporotic patient. This finding may be a harbinger of poor healing capacity that should be considered when directing any potential surgical intervention. Urologic injury is estimated to be present in 15% to 45% of all pelvic ring injuries, but this is typically confined to high-energy lateral compression and anteroposterior compression injuries. All of these issues must be considered in planning treatment.
Evaluation of the patient with osteoporotic pelvic trauma
Mechanism of Injury
The large majority of osteoporotic pelvic ring injuries result from low-energy mechanisms; however, this should not be assumed. With the increased incidence of older patients driving and working, the possibility arises that their trauma is the result of high energy. A careful history along with a description of the scene and understanding of any other injuries that may have occurred to other patients are key considerations.
Low-Energy Pelvic Ring Injuries
A fall from a standing position is the most common mechanism for an osteoporotic patient presenting with a pelvic ring injury. Often these patients are unable to ambulate and are evaluated in an emergency department setting. A careful history and physical examination is paramount. These patients may present with marked dementia and are unable to effectively communicate. In addition, they might suffer from medical conditions that predispose them to bony injury. For example, the growing population with rheumatoid arthritis incurs a 1.5-times higher rate of fracture than age-matched controls. This history may also influence the decision-making tree in treatment, as patients may be on medications that can interfere with wound healing and anesthesia. Some critical points in the medical history that deserve special consideration include a history of malignancy in the pelvis requiring radiation, a history of surgery in the lumbar spine requiring dorsal bone grafting, and a history of treatment for osteoporosis.
A complete physical examination should include a focused neurologic evaluation, as comminuted fractures of the posterior pelvic ring often will injure the exiting nerve roots to varying degrees. In addition, a careful evaluation of the skin is required, as disruption may occur owing to poor quality, as well as a clinical evaluation of leg length. Radiographic evaluation should begin with an anteroposterior view of the pelvis. The most common findings of fracture on this image will be of the superior and inferior pubic ramus. The constellation of rami fractures along with their individual orientation may predict potential displacement, which should elicit further evaluation with inlet and outlet radiographs, computed tomography (CT) imaging, or both. The latter is particularly important for evaluation of the posterior pelvic ring, where it is estimated that 30% of pelvic ring injuries are missed without the combination of both CT and plain radiography. The most common bony injury in the posterior pelvis is a fracture of the sacrum lateral to the foramina and medial to the sacroiliac joint. This fracture line is usually incomplete, but should be examined on the coronal CT format to determine if the fracture indeed exits the posterior sacrum. The key point in radiographic evaluation, however, is that there is rarely injury to the pelvic ligaments in osteoporotic patients because the strength of these ligaments exceeds that of the osteoporotic pelvic bone. As such, a severe bony injury from a low-energy mechanism may be stable and does not warrant surgical intervention. Recognition of potential bilateral vertical sacral fractures connected through disc spaces or vertebral bodies, which will often occur through a severely degenerated region of the bone, can change treatment recommendations significantly. These fractures may represent the high-energy variant in young patients known as spinopelvic dissociation. In addition, evaluation of the lumbar spine and pelvic ring for periprosthetic fractures in the presence of existing hardware can be accomplished by CT. Examples might include disruption of a pedicle around a screw placed during a prior lumbar fusion procedure, or a periprosthetic acetabular fracture around a pubic root fracture. Discovery of such injuries may affect surgical planning.
A more complex group of patients with low-energy pelvic ring fracture are those with suspected altered biomechanics attributable to a myriad of causes that essentially allow for insufficiency fractures, particularly of the sacrum but also of the rami. Often these fractures are discovered accidentally, and the risk factors identified have included osteoporosis, rheumatoid arthritis, corticosteroid treatment, and mechanical constraint from prior instrumentation. These fractures are often not identified immediately, and a delay in diagnosis can range from 1 to 3 months. Magnetic resonance imaging in a patient with negative physical and plain radiography findings, but recalcitrant low back pain, may yield the diagnosis and allow for careful treatment.
Treatment of low-energy fractures
The patient with low-energy pelvic fracture may have a radiograph with fracture patterns that appear to fit into the Young and Burgess or the Tile classification systems, but the treatment varies widely because the mechanisms do not impart nearly the same energy into the pelvic ring. Therefore, the classification of these injuries in the same systems used for high-energy fracture is questionable. Hemodynamic instability secondary to the fracture is also rarely present on presentation, so the use of pelvic binders, sheets, C-clamps, and external fixators is rarely indicated. In fact the use of a C-clamp may be directly contraindicated by the insufficiency of the posterior pelvis in avoiding iatrogenic injury.
The tenet of treatment for all osteoporotic fractures is early mobilization. It is well known that extended periods of bed rest will lead to pneumonia, decubitus ulceration, deep venous thrombosis and, in the case of the pelvis, will often not lead to avoidance of a subsequent deformity. This evidence is extrapolated from data on fractures of the proximal femur, for which early mobilization has become the gold standard.
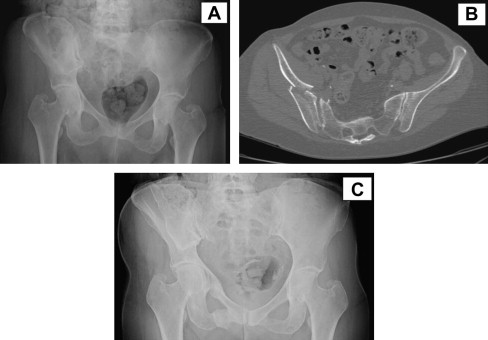
Ideally the patient should be treated with minimized weight bearing with an assistive device on the affected side. Given their advanced age and risk for falls, many osteoporotic patients are maintained as weight bearing as tolerated, with appropriate analgesics and venothromboembolic prophylaxis (pharmacologic and mechanical). Some authors have recommended postmobilization imaging to visualize fractures that potentially might not have been easily visualized on initial radiographs or even CT, owing to the marked osteoporotic changes ( Fig. 1 ). If patients are unable to mobilize effectively for reasons of pain control, it has been postulated that compression of the posterior pelvic ring (sacral fracture) can lead to decreased pain and increased ambulatory capacity. The relative osteoporotic sacral vertebral bodies do not contain bone stock adequate enough to achieve compression across the sacral fracture, therefore the use of long-screw fixation known as transsacral screw fixation, which traverses the entire sacrum and engages the contralateral ilium, is recommended. This type of fixation is technically demanding and requires familiarity with the technique so as to avoid iatrogenic injury to neurovascular structures. Alternatively, if the fracture is contained to zone I of the sacrum and is nondisplaced, there is growing support for the use of sacroplasty whereby bone cement is injected percutaneously into the region of the fracture to fill in the defect created by the fracture. Significant pain relief is noted, similar to vertebroplasty, and the opportunity to augment the cement with iliosacral or transsacral screw fixation remains a viable option. A question that has not been answered is whether the use of calcium phosphate or calcium sulfate bone substitutes in this region would provide improved incorporation and the ability to insert screws for fixation rather than cement.
Related posts:
 Osteoporosis and Fragility Fractures
Osteoporosis Diagnosis and Medical Treatment
Surgical Stabilization of the Spine in the Osteoporotic Patient
Managing Atrophic Nonunion in the Geriatric Population
Bisphosphonate Therapy and Atypical Fractures
Surgical Stabilization of the Spine in the Osteoporotic Patient
Osteoporosis and Fragility Fractures
Osteoporosis Diagnosis and Medical Treatment
Surgical Stabilization of the Spine in the Osteoporotic Patient
Managing Atrophic Nonunion in the Geriatric Population
Bisphosphonate Therapy and Atypical Fractures
Surgical Stabilization of the Spine in the Osteoporotic Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


