 FIGURE 34-1 Unstable lesion that requires fixation. |
condyle (Fig. 34-2). The size of the lesion usually can be accurately determined on plain radiographs. Most small lesions are stable; lesions with a sclerotic margin of 3 mm or more and lesions larger than 0.8 cm2 have an increased risk of being loose. Comparison radiographs should be obtained in juvenile and adolescent patients because an OCD lesion may be confused with ossification centers, which may cause transient symptoms but usually resolve spontaneously within 6 to 12 months. In addition, OCD is bilateral in approximately 30% of patients (Fig. 34-3).
TABLE 34-1. Surgical Treatment Options for Osteochondritis Dissecans of the Femoral Condyle | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||
(Fig. 34-4). Currently, a spoiled gradient (SPGR) echo sequence using fat suppression and three-dimensional acquisition is considered the optimal technique for evaluating articular cartilage lesions. The presence of fluid around the fragment or focal cystic areas beneath the fragment is the best indicator of instability; the absence of a zone of high-signal intensity at the interface of the fragment and the bone is a reliable sign of lesion stability (28). Magnetic resonance imaging also is useful for identification of associated ligamentous and meniscal injuries.
 FIGURE 34-2 Recommended radiographic views for evaluation of OCD of the knee. A: Anteroposterior. B: Lateral. C: Tunnel. |
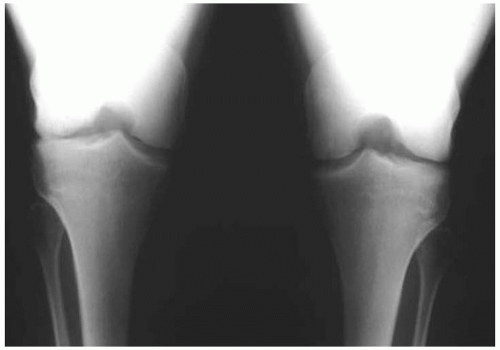 FIGURE 34-3 Bilateral OCD lesions of lateral femoral condyles. |
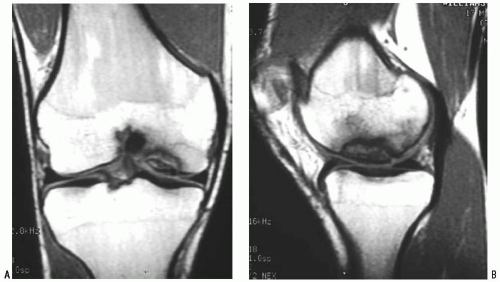 FIGURE 34-4 MRI evaluation of OCD. A: AP-coronal plane view. B: Lateral sagittal plane view. |
Typically, a 30-degree arthroscope is used, although a 70-degree arthroscope can sometimes be helpful when the lesion is posterior.
A complete and systematic examination of the joint with the 30-degree arthroscope in the anterolateral portal is the first step in any arthroscopic procedure about the knee. The articular surfaces of the femoral condyles should be inspected carefully. Moving the knee from 20 to 90 degrees of flexion during viewing will help with inspection of the posterior extent of the lesion.Related posts:
 Patella and/or Extensor Mechanism Allograft Reconstruction
Patella and/or Extensor Mechanism Allograft Reconstruction
 Acute Quadriceps Tendon Repair
Acute Quadriceps Tendon Repair
 Anterior Cruciate Ligament Reconstruction
Anterior Cruciate Ligament Reconstruction
 Arthroscopically Assisted Posterior Cruciate Ligament Reconstruction
Arthroscopically Assisted Posterior Cruciate Ligament Reconstruction
 Microfracture Technique: Treatment of Full-Thickness Chondral Lesions
Microfracture Technique: Treatment of Full-Thickness Chondral Lesions
 Allograft Transplantation for Articular Defects of the Knee
Allograft Transplantation for Articular Defects of the Knee

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


